

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Review
Volume 8, Number 12, December 2016, pages 848-853
Exercise Intervention for Anti-Sarcopenia in Community-Dwelling Older People
Ryo Miyazakia, Taro Takeshimab, Kazuhiko Kotanib, c
aDepartment of Sports and Health Sciences, Faculty of Human Sciences, University of East Asia, Yamaguchi, Japan
bDivision of Community and Family Medicine, Jichi Medical University, Tochigi, Japan
cCorresponding Author: Kazuhiko Kotani, Division of Community and Family Medicine, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke City, Tochigi 329-0498, Japan
Manuscript accepted for publication September 29, 2016
Short title: Exercise Intervention for Anti-Sarcopenia
doi: http://dx.doi.org/10.14740/jocmr2767w
| Abstract | ▴Top |
Sarcopenia is an age-related health problem in general communities. Effective exercise programs against sarcopenia remain necessary for community-dwelling older people. In order to summarize the available knowledge on this subject, we collected English articles from a MEDLINE/Pubmed database examining the effects of exercise interventions on sarcopenia-related outcome measures in community-dwelling older people. When nine articles, including eight randomized controlled trials, were reviewed, most studies demonstrated significant improvements in some outcome measures. Indeed, a significant improvement in the muscle mass in one study, muscle strength in two studies and physical performance in two studies was reported among five studies using exercise (E) alone. A significant improvement in the muscle mass in two studies, muscle strength in one study and physical performance in two studies was also reported among four studies using exercise plus nutritional supplementation (EN). Notably, the EN studies appeared to have less extensive exercise interventions than the E studies. One EN study further exhibited significant improvements in all outcome measures. Collectively, exercise could be used as anti-sarcopenic strategies and nutritional interventions when combined with exercise might play a compensated or perhaps a comprehensive role among community-dwelling older people. Limited studies exist and more studies are required for the optimum programs in the community settings.
Keywords: Skeletal muscle; Training; Nutritional supplementation; Elderly
| Introduction | ▴Top |
Sarcopenia reduces skeletal muscle mass/strength among older people, which induces physical dysfunction and age-related diseases [1-3]. As the aging of societies is progressing worldwide, sarcopenia is now commonly seen in general communities; indeed, the community-based prevalence of sarcopenia is reported to be either 4.1-11.5% [4] or 5-13% [5] in those ≥ 65 years of age and 11-50% in those ≥ 80 years of age [5]. Thus, strategies to prevent and manage sarcopenia among community-dwelling older people are currently in great demand.
Exercise is considered an essential strategy against sarcopenia [4], and several exercise intervention programs against sarcopenia (onset and/or progression) have been deployed in the community settings. Furthermore, the addition of nutritional intervention to exercise intervention has recently been debated for anti-sarcopenia [4, 6, 7]. Because community-dwelling people have certain characteristics, such as being in good physical condition compared to patients at the clinic and hospital levels, community-focused intervention programs should be developed. However, previous reviews have been performed in mixed populations including both patients as well as the general populations [6, 7].
Summarizing articles examining the anti-sarcopenic effects of exercise interventions restricted to community-dwelling older people would be useful for developing strategies targeting this particular population. We herein aimed to summarize the available knowledge on this subject.
| Methods | ▴Top |
Search strategy
The electronic database Medical Literature Analysis and Retrieval System Online MEDLINE/Pubmed was applied to search for articles published up to June 2016. The following keywords were used: sarcopenia, intervention, physical activity, elderly and community.
Literature selection
Studies in human trials of exercise interventions against sarcopenia were collected for the present review. Full-length original articles written in English were eligible. With regard to the study design, randomized control trials (RCTs) and non-randomized control trials (nRCTs; single-arm trials or comparative control trials) were eligible. Articles on exercise interventions accompanied by nutritional supplementations were deemed eligible so long as the study considered the anti-sarcopenic effects of exercise. The current definitions of sarcopenia in Europe [8] and Asia [9] are as follows: 1) age ≥ 65 years and 2) presence of muscle loss as well as low muscle strength and/or physical performance (i.e. gait speed). Therefore, the articles that examined sarcopenia-related outcome measures of muscle mass, muscle strength and/or physical performance, including gait speed, were eligible for the present review. We excluded the articles that experimentally examined muscle metabolism only (e.g. muscle fiber and protein synthesis).
Based on the criteria, the titles and abstracts of the articles were screened independently by two investigators. The investigators further evaluated the full-text articles and finally determined their inclusion in the present review.
| Results | ▴Top |
Study selection
Of the initial 27 studies retrieved, 19 were evaluated for eligibility. Ten articles were further excluded for the following reasons (Fig. 1): the study subjects were not necessarily older people (two articles), the study did not assess the sarcopenia-related outcome measures (three articles), the study design was cross-sectional (two articles), the study was not based on exercise interventions (two articles) and only the study protocol was described without any interventional results (one article). Although three articles used the same study populations, they were included in this review as independent articles because the respective articles had different study purposes and results. Ultimately, a total of nine articles were included in our review, as shown in Table 1 [10-18].
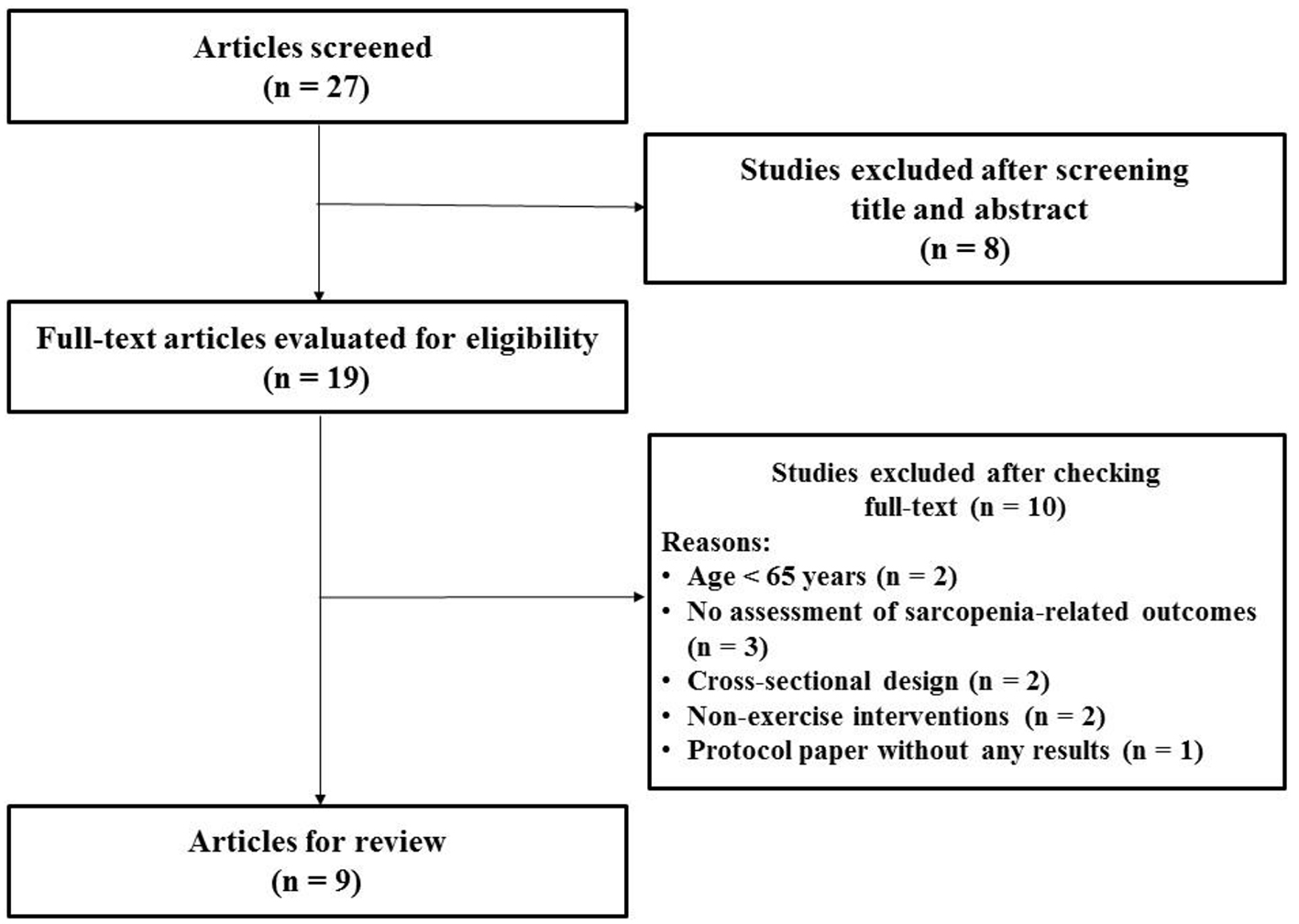 Click for large image | Figure 1. Flow diagram of study selection. |
 Click to view | Table 1. A Summary of the Exercise and Exercise Plus Nutritional Supplementation Interventions |
Study designs
Eight studies were RCTs [10-17] and one was a single-arm trial [18]. Of the eight RCTs, one was analyzed retrospectively [18]. Five of the studies were based on interventions of exercise (E) alone [10-13, 18], and four were based on interventions of exercise plus nutritional supplementation (EN) [14-17]. One study had two comparison groups (with two different forms of exercise interventions) [13], and four studies compared outcomes among three to four groups (exercise, nutritional supplementation or exercise plus nutritional supplementation vs. control groups) [14-17].
All of the studies were carried out in the community settings. Four studies were conducted in the USA [10, 11, 13, 18], two in Europe (Germany and Sweden) [12, 17] and the others in Japan [14-16].
Study populations
All study subjects were community-dwelling older people ≥ 65 years of age. As mentioned above, the three studies (called the LIFE study) used the same study populations [10, 11, 13]. The number of study subjects varied widely, from 57 [13] to 1,635 [10]. Five of the studies were conducted among subjects of both genders [10, 11, 14, 17, 18], while the remaining studies were conducted in females only. One study [13] described no information regarding the gender.
The subjects were recruited using the following various methods: a local press advertisement [14], flyers [18], invitation letters [15, 16], as well as in-person explanations in local field centers [10, 11, 13], residential care facilities [17] and university ambulatory sections [12]. These subjects were general people [10, 12, 14, 18] but also included partially a special population, for instance with sarcopenia [15, 16] and with mobility disability [11, 13, 17].
Interventions
As shown in Table 1, five studies [10-12, 15, 16] employed mixed exercise forms (i.e. aerobic, resistance, flexibility and balance training). These five studies used resistance training in particular. One study compared two resistance training forms (high-velocity high-power vs. a traditional slow-velocity progressive resistance training form) [13]. In the other two studies, resistance training using resistance bands [18] and focusing on improving lower-limb strength [17] were employed. One study used aerobic training [14].
The exercise frequencies ranged between 2 and 7 days/week and 1 and 14 sessions/week across studies [10-18], although the frequencies were generally considered to be at least 2 days/week. In particular, the exercise frequencies appeared to be lower in the EN studies than in the E studies, and even when the exercise training was frequently provided in an EN study [14], the content of the exercise was at walking level. In addition, the exercise training was not always provided at the studied centers. Four studies combined the center-based training with supervised trainers and home-based training [10-13].
Four studies combined interventions of exercise with nutritional supplements. The supplementation was delivered as follows: tea catechin [15], amino acid [16], amino acid (mainly leucine) and protein-enriched drink [17] and protein and vitamin D [14].
Adherence to interventions
Six studies reported retention rates regarding adherence to the intervention. The rates were all over 70%, ranging from 70.3% [16] to 97.8% [14].
Sarcopenia-related outcomes
As sarcopenia-related outcome measures, muscle mass (i.e., muscle area, lean mass, fat free mass) was evaluated in seven studies [11-17], muscle strength was studied in five studies [11, 13, 16, 18] and physical performance (i.e. gait speed) was studied in four studies [11, 15, 16, 18]. In the E studies, as shown in Table 1, all studies except one showed significant improvements in some sarcopenia-related outcome measures [11]; namely, one study described a significant increase (improvement) in muscle mass [12], two described a significant increase (improvement) in muscle strength [13, 18] and two described a significant improvement in physical performance [10, 18]. Similarly, in the EN studies, all studies except one also showed significant improvements in some sarcopenia-related outcome measures [17]; namely, two studies described a significant increase in muscle mass [14, 16], one described a significant increase in muscle strength [16] and two described a significant improvement in physical performance [15, 16]. Although one study described no marked changes in the measures (muscle mass) with protein-enriched supplementation [17], the other studies noted significant improvement in at least one outcome measure with supplementation via tea catechin [15], amino acid alone [16] and protein and vitamin D [14]. One EN study [16] in particular showed improvements in all outcome measures, including muscle mass, muscle strength and physical performance (gait speed).
Overall, the studies using resistance training forms showed an increasing (improving) trend in muscle strength [13, 18], while those using mixed training forms showed an increasing (improving) trend in physical performance [10, 15, 16]. The studies with greater exercise frequencies (≥ 2 - 3 times/week) showed an increasing (improving) trend in muscle mass/strength [10, 12, 13, 18].
| Discussion | ▴Top |
The present review focusing on community-dwelling older people demonstrated that exercise and exercise plus nutritional interventions could significantly improve some sarcopenia-related outcome measures, suggesting the interventions to be effective as an anti-sarcopenic strategy among such people. The anti-sarcopenic effects were found to be largely similar between the E and EN studies, while the EN interventions appeared to have less extensive exercise interventions than the E interventions. These findings obtained mainly from RCTs can be useful, while there remains to be a difficult situation due to limited studies on this subject in order to develop effective strategies against sarcopenia in the community settings.
The finding of the anti-sarcopenic effects of exercise in the present review confirms its usefulness against sarcopenia, as described previously [4]. This is natural, as sarcopenia is based on skeletal muscle pathologies [1, 2]. Mechanistically, exercise is known to counter sarcopenia by reducing levels of inflammatory cytokines that induce muscle damage [19] as well as stimulation of the rates of protein synthesis and suppression of the breakdown in muscle cells [20].
Recently, the addition of nutritional intervention to exercise has received focus with respect to its utility in anti-sarcopenia [4, 6, 7]. A poor nutritional status is recognized to be associated with not only muscle disorders but also physical dysfunction in older people [7]. The present review indicated seemingly similar anti-sarcopenic effects when combining nutritional supplementation with exercise to exercise alone. Of note, the anti-sarcopenic effects might exist by less extensive exercise contents in exercise plus nutritional interventions relative to exercise alone. The addition of nutritional intervention to exercise may therefore have a compensatory anti-sarcopenic effect, for example in subjects with insufficient exercise. Furthermore, while evidence to this was obtained in only one study in the present review [16], a comprehensive effect (an improvement in all measures, including physical performance) might also exist. This finding may mean that the effects of exercise plus nutritional intervention are not achievable by exercise alone.
The anti-sarcopenic effects can differ depending on nutritional supplementation when combined with exercise, and a greater benefit was proposed by protein/amino acid and multi-nutrient supplements [6]. However, in the present review, exercise with protein-enriched supplementation did not always show the improvements in sarcopenia-related outcome measures [17]. Although the reason for this is not entirely clear at present, the characteristics of the study populations (e.g. community-dwelling people are in relatively healthy conditions) may have played some roles; as such, more studies regarding the effects of combination of exercise with nutritional supplements are required in the community settings.
We observed a trend wherein resistance training improved the muscle strength and mixed training improved the physical performance. Resistance training induces muscle constriction and hypertrophy, thereby improving muscle strength [21]. Low-intensity resistance training with slow movements has been recently reported to be as effective as traditional (heavily loaded with a faster speed) resistance training in improving muscle strength [22, 23]. In addition, as resistance training induces protein synthesis and aerobic training reduces protein breakdown in muscle tissues [24-26], the superiority of mixed training to resistance training in improving a wide range of physical conditions has been assumed, on considering muscle pathologies. Therefore, various training forms should be applied in exercise interventions for anti-sarcopenia. Since such trainings do not require expensive machines to perform, light-to-moderate resistance or mixed training can be easily applied in anti-sarcopenic exercise interventions in the community settings. The influence of the ease-of-use of such trainings also seemed to be reflected in the relatively high rates of adherence to the interventions across the studies in the present review (Table 1). Furthermore, the present review indicated a greater exercise frequency (≥ 2 - 3 times/week) to be crucial for anti-sarcopenia. This frequency is thought to concur with the current consensus regarding resistance training as described in the guidelines by the American College of Sports Medicine [27].
Several limitations associated with the present study warrant mention. First, our review compiled the results of limited studies. Second, there was heterogeneity across the studies in terms of the intervention durations and intervention methods. Thus, caution should be practiced when interpreting and generalizing the findings. Moreover, in order to study the community-oriented anti-sarcopenic interventions, the additional measures that are related to sarcopenia but not examined in the studies included in the present review (e.g. the knowledge level of sarcopenia and socioeconomic status at the community level) [28-30] should be considered as a future issue.
| Conclusions | ▴Top |
The present review of studies conducted in the community settings showed that exercise and exercise plus nutritional interventions could be effective for anti-sarcopenia among community-dwelling older people. The anti-sarcopenic effects of exercise alone and in combination with nutritional supplementation were largely similar, with implications of a compensated or perhaps comprehensive role of nutritional interventions when combined with exercise. Limited studies exist and more studies are warranted to establish the optimum anti-sarcopenic strategies using exercise in the general community.
| Conflicts of Interest | ▴Top |
The authors declare no conflicts of interest with respect to the research, authorship and publication of this article.
| References | ▴Top |
- Doherty TJ. Invited review: Aging and sarcopenia. J Appl Physiol (1985). 2003;95(4):1717-1727.
doi pubmed - Beaudart C, Reginster JY, Slomian J, Buckinx F, Dardenne N, Quabron A, Slangen C, et al. Estimation of sarcopenia prevalence using various assessment tools. Exp Gerontol. 2015;61:31-37.
doi pubmed - De Spiegeleer A, Petrovic M, Boeckxstaens P, Van Den Noortgate N. Treating sarcopenia in clinical practice: where are we now? Acta Clinica Belgica. 2016;71:197-205.
- Chen LK, Lee WJ, Peng LN, Liu LK, Arai H, Akishita M. Recent Advances in Sarcopenia Research in Asia: 2016 Update From the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2016;17(8):767 e761-767.
- Abellan van Kan G. Epidemiology and consequences of sarcopenia. J Nutr Health Aging. 2009;13(8):708-712.
doi pubmed - Denison HJ, Cooper C, Sayer AA, Robinson SM. Prevention and optimal management of sarcopenia: a review of combined exercise and nutrition interventions to improve muscle outcomes in older people. Clin Interv Aging. 2015;10:859-869.
pubmed - Artaza-Artabe I, Saez-Lopez P, Sanchez-Hernandez N, Fernandez-Gutierrez N, Malafarina V. The relationship between nutrition and frailty: Effects of protein intake, nutritional supplementation, vitamin D and exercise on muscle metabolism in the elderly. A systematic review. Maturitas. 2016.
doi pubmed - Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412-423.
doi pubmed - Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, Chou MY, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95-101.
doi pubmed - Sink KM, Espeland MA, Castro CM, Church T, Cohen R, Dodson JA, Guralnik J, et al. Effect of a 24-Month Physical Activity Intervention vs Health Education on Cognitive Outcomes in Sedentary Older Adults: The LIFE Randomized Trial. JAMA. 2015;314(8):781-790.
doi pubmed - Liu CK, Leng X, Hsu FC, Kritchevsky SB, Ding J, Earnest CP, Ferrucci L, et al. The impact of sarcopenia on a physical activity intervention: the Lifestyle Interventions and Independence for Elders Pilot Study (LIFE-P). J Nutr Health Aging. 2014;18(1):59-64.
doi pubmed - Kemmler W, von Stengel S. Exercise frequency, health risk factors, and diseases of the elderly. Arch Phys Med Rehabil. 2013;94(11):2046-2053.
doi pubmed - Reid KF, Callahan DM, Carabello RJ, Phillips EM, Frontera WR, Fielding RA. Lower extremity power training in elderly subjects with mobility limitations: a randomized controlled trial. Aging Clin Exp Res. 2008;20(4):337-343.
doi pubmed - Yamada M, Nishiguchi S, Fukutani N, Aoyama T, Arai H. Mail-Based Intervention for Sarcopenia Prevention Increased Anabolic Hormone and Skeletal Muscle Mass in Community-Dwelling Japanese Older Adults: The INE (Intervention by Nutrition and Exercise) Study. J Am Med Dir Assoc. 2015;16(8):654-660.
doi pubmed - Kim H, Suzuki T, Saito K, Yoshida H, Kojima N, Kim M, Sudo M, et al. Effects of exercise and tea catechins on muscle mass, strength and walking ability in community-dwelling elderly Japanese sarcopenic women: a randomized controlled trial. Geriatr Gerontol Int. 2013;13(2):458-465.
doi pubmed - Kim HK, Suzuki T, Saito K, Yoshida H, Kobayashi H, Kato H, Katayama M. Effects of exercise and amino acid supplementation on body composition and physical function in community-dwelling elderly Japanese sarcopenic women: a randomized controlled trial. J Am Geriatr Soc. 2012;60(1):16-23.
doi pubmed - Carlsson M, Littbrand H, Gustafson Y, Lundin-Olsson L, Lindelof N, Rosendahl E, Haglin L. Effects of high-intensity exercise and protein supplement on muscle mass in ADL dependent older people with and without malnutrition: a randomized controlled trial. J Nutr Health Aging. 2011;15(7):554-560.
doi pubmed - Abreu EL, Cheng AL, Kelly PJ, Chertoff K, Brotto L, Griffith E, Kinder G, et al. Skeletal muscle troponin as a novel biomarker to enhance assessment of the impact of strength training on fall prevention in the older adults. Nurs Res. 2014;63(2):75-82.
doi pubmed - Beyer I, Mets T, Bautmans I. Chronic low-grade inflammation and age-related sarcopenia. Curr Opin Clin Nutr Metab Care. 2012;15(1):12-22.
doi pubmed - Yarasheski KE. Exercise, aging, and muscle protein metabolism. J Gerontol A Biol Sci Med Sci. 2003;58(10):M918-922.
doi pubmed - Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci. 2006;61(10):1059-1064.
doi pubmed - Tanimoto M, Sanada K, Yamamoto K, Kawano H, Gando Y, Tabata I, Ishii N, et al. Effects of whole-body low-intensity resistance training with slow movement and tonic force generation on muscular size and strength in young men. J Strength Cond Res. 2008;22(6):1926-1938.
doi pubmed - Watanabe Y, Madarame H, Ogasawara R, Nakazato K, Ishii N. Effect of very low-intensity resistance training with slow movement on muscle size and strength in healthy older adults. Clin Physiol Funct Imaging. 2014;34(6):463-470.
doi pubmed - Roubenoff R, Hughes VA. Sarcopenia: current concepts. J Gerontol A Biol Sci Med Sci. 2000;55(12):M716-724.
doi pubmed - Konopka AR, Douglass MD, Kaminsky LA, Jemiolo B, Trappe TA, Trappe S, Harber MP. Molecular adaptations to aerobic exercise training in skeletal muscle of older women. J Gerontol A Biol Sci Med Sci. 2010;65(11):1201-1207.
doi pubmed - Harber MP, Konopka AR, Jemiolo B, Trappe SW, Trappe TA, Reidy PT. Muscle protein synthesis and gene expression during recovery from aerobic exercise in the fasted and fed states. Am J Physiol Regul Integr Comp Physiol. 2010;299(5):R1254-1262.
doi pubmed - American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687-708.
doi pubmed - Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380(9838):258-271.
doi - Alexandre Tda S, Duarte YA, Santos JL, Wong R, Lebrao ML. Prevalence and associated factors of sarcopenia among elderly in Brazil: findings from the SABE study. J Nutr Health Aging. 2014;18(3):284-290.
doi pubmed - Laussen J, Kowaleski C, Martin K, Hickey C, Fielding RA, Reid KF. Disseminating a Clinically Effective Physical Activity Program to Preserve Mobility in a Community Setting for Older Adults. J Frailty Aging. 2016;5(2):82-87.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.