

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://www.jocmr.org |
Original Article
Volume 15, Number 5, May 2023, pages 262-267

Characteristics of Patients With Inflammatory Bowel Disease Who Develop Bloodstream Infection
Mitsuhiro Kamadaa, d, e, Motoyasu Miyazakia, d, Akio Nakashimaa, Yota Yamadaa, Takafumi Nakanob, Daiki Hagiwarab, Yukie Komiyac, Koichi Matsuoa, Osamu Imakyurea
aDepartment of Pharmacy, Fukuoka University Chikushi Hospital, Fukuoka 818-8502, Japan
bDepartment of Pharmacy, Fukuoka University Hospital, Fukuoka 814-0180, Japan
cDepartment of Clinical Laboratory, Fukuoka University Chikushi Hospital, Fukuoka 818-8502, Japan
dThese authors contributed equally to this work.
eCorresponding Author: Mitsuhiro Kamada, Department of Pharmacy, Fukuoka University Chikushi Hospital, Fukuoka 818-8502, Japan
Manuscript submitted April 11, 2023, accepted May 29, 2023, published online May 31, 2023
Short title: Characteristics of IBD Patients With BSI
doi: https://doi.org/10.14740/jocmr4920
| Abstract | ▴Top |
Background: The causative microorganisms of bloodstream infections (BSIs) in patients with inflammatory bowel disease (IBD) and the clinical characteristics of these patients have not yet been fully identified. Therefore, this study investigated IBD patients who developed BSI to determine their clinical characteristics and identify the BSI-causing bacteria.
Methods: The subjects were IBD patients who developed bacteremia between 2015 and 2019 at Fukuoka University Chikushi Hospital. The patients were divided into two groups according to IBD type (Crohn’s disease (CD) or ulcerative colitis (UC)). The medical records of the patients were reviewed to determine their clinical backgrounds and identify the BSI-causing bacteria.
Results: In total 95 patients, 68 CD and 27 UC patients were included in this study. The detection rates of Pseudomonas aeruginosa (P. aeruginosa) and Klebsiella pneumoniae (K. pneumoniae) were higher in the UC group than in the CD group (18.5% vs. 2.9%, P = 0.021; 11.1% vs. 0%, P = 0.019, respectively). Immunosuppressive drugs use was higher in the CD group than in the UC group (57.4% vs. 11.1%, P = 0.00003). Hospital stay length was longer in the UC group than in the CD group (15 vs. 9 days; P = 0.045).
Conclusions: The causative bacteria of BSI and clinical backgrounds differed between patients with CD and UC. This study showed that P. aeruginosa and K. pneumoniae had higher abundance in UC patients at the onset of BSI. Furthermore, long-term hospitalized patients with UC required antimicrobial therapy against P. aeruginosa and K. pneumoniae.
Keywords: Crohn’s disease; Ulcerative colitis; Bloodstream infection
| Introduction | ▴Top |
Inflammatory bowel disease (IBD) is an intractable disease that presents with symptoms such as mucous stool, diarrhea, and abdominal pain due to immune and organic abnormalities in the intestinal tract [1]. IBD is broadly divided into Crohn’s disease (CD) and ulcerative colitis (UC). In CD, the entire gastrointestinal tract from the mouth to the anus is inflamed, whereas in UC, only the innermost layer of the intestinal wall in the colon is superficially inflamed [2]. Although the intestinal tract has defense mechanisms against pathogens in the intestinal flora and other bacteria [3], patients with IBD have reduced intestinal immunity with complex interactions between the intestinal flora and host immune function [4, 5]. Therefore, IBD is known to be a risk factor for developing bloodstream infection (BSI) [6].
BSI is a high mortality condition that is often seen in healthcare settings. BSI can occur when bacteria enter the bloodstream (i.e., bacteremia), which can lead to sepsis and death. Both gram-positive and gram-negative bacteria are known to cause bacteremia. Understanding the causative organisms of BSI is thought to help reduce patient mortality [7], but differences between the BSI-causing bacteria in CD and UC patients have not been fully elucidated. Although IBD has been listed as a causative agent of bacteremia [8], there remain no large-scale epidemiological data specific to IBD patients. A better understanding of the cause of BSI in CD and UC patients could help determine the initial treatment needed in IBD patients with BSI. The aim of this study was to compare the causative organisms and clinical backgrounds of blood isolates from CD and UC patients from a single medical center.
| Materials and Methods | ▴Top |
Study design and survey items
The study subjects were IBD patients who developed bacteremia between 2015 and 2019 at Fukuoka University Chikushi Hospital, Fukuoka, Japan. We retrospectively evaluated the age, sex, patient background, body mass index (BMI), length of hospital stay, use of immunosuppressants and blood culture results in each case using our electronic medical records. Immunosuppressant users were defined as those who used one of the following six drugs for IBD treatment: infliximab, azathioprine, mercaptopurine, methotrexate, adalimumab, or prednisolone. Patients who did not receive two sets of blood cultures were excluded. This study was approved by the Fukuoka University-Medical Ethics Review Board (approval number C20-05-004). All methods were performed in accordance with the relevant guidelines and regulations.
Bacterial isolate
IBD patients who developed bacteremia after an interval of 3+ months were considered blood culture-positive patients for this study. For each patient, blood cultures were submitted, and the presence or absence of infectious disease-causing factors were verified under a microscope by smear examination. We also reproduced suspected infected lesions by culturing bacteria to confirm whether there was a causative bacterium. The blood culture positive patients were split into two groups based on their IBD type (CD or UC).
Statistical analysis
To compare the CD and UC patients, the Wilcoxon rank sum test was used to compare the medians between the two groups and the Fisher’s exact test was used to compare their frequency differences. The values in the text are given as the median (interquartile range). Patients with a risk rate of < 5% were considered significantly different. JMP statistical analysis software (version 10.0.2; SAS Inc., Tokyo, Japan) was used for all statistical analyses.
| Results | ▴Top |
During the study period, 905 patients developed BSI. Of these, 109 had IBD. Fourteen patients who did not receive two sets of blood cultures were excluded. In total, 68 CD and 27 UC patients were included in this study (Fig. 1). Staphylococcus epidermidis (S. epidermidis) was the most frequently detected gram-positive bacteria among all included patients. Escherichia coli (E. coli) and Enterobacter sp. had the highest ratios, respectively, for the gram-negative bacteria (Fig. 2).
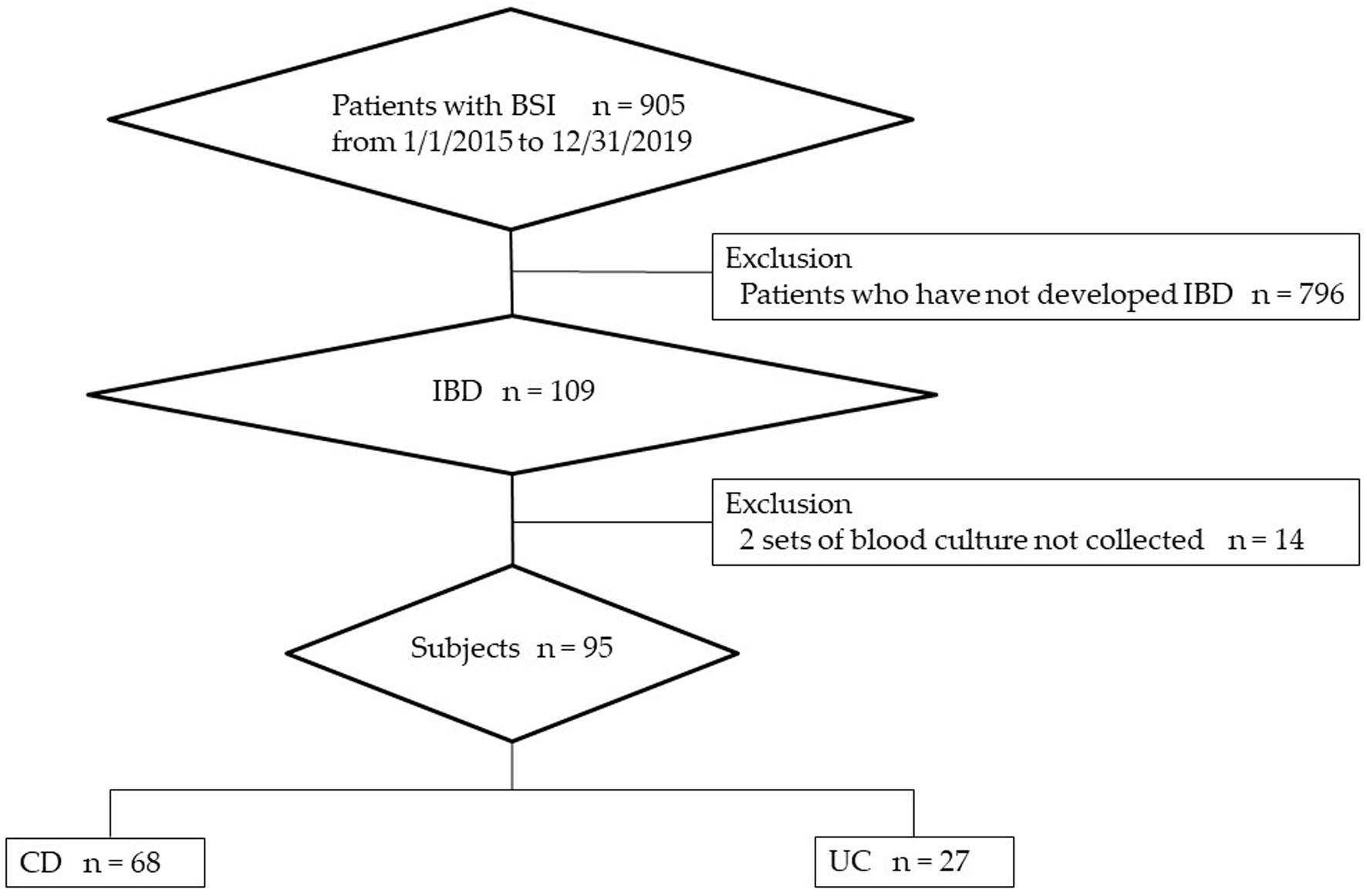 Click for large image | Figure 1. IBD patients with BSI during the study period. BSI: bloodstream infection; CD: Crohn’s disease; IBD: inflammatory bowel disease; UC: ulcerative colitis. |
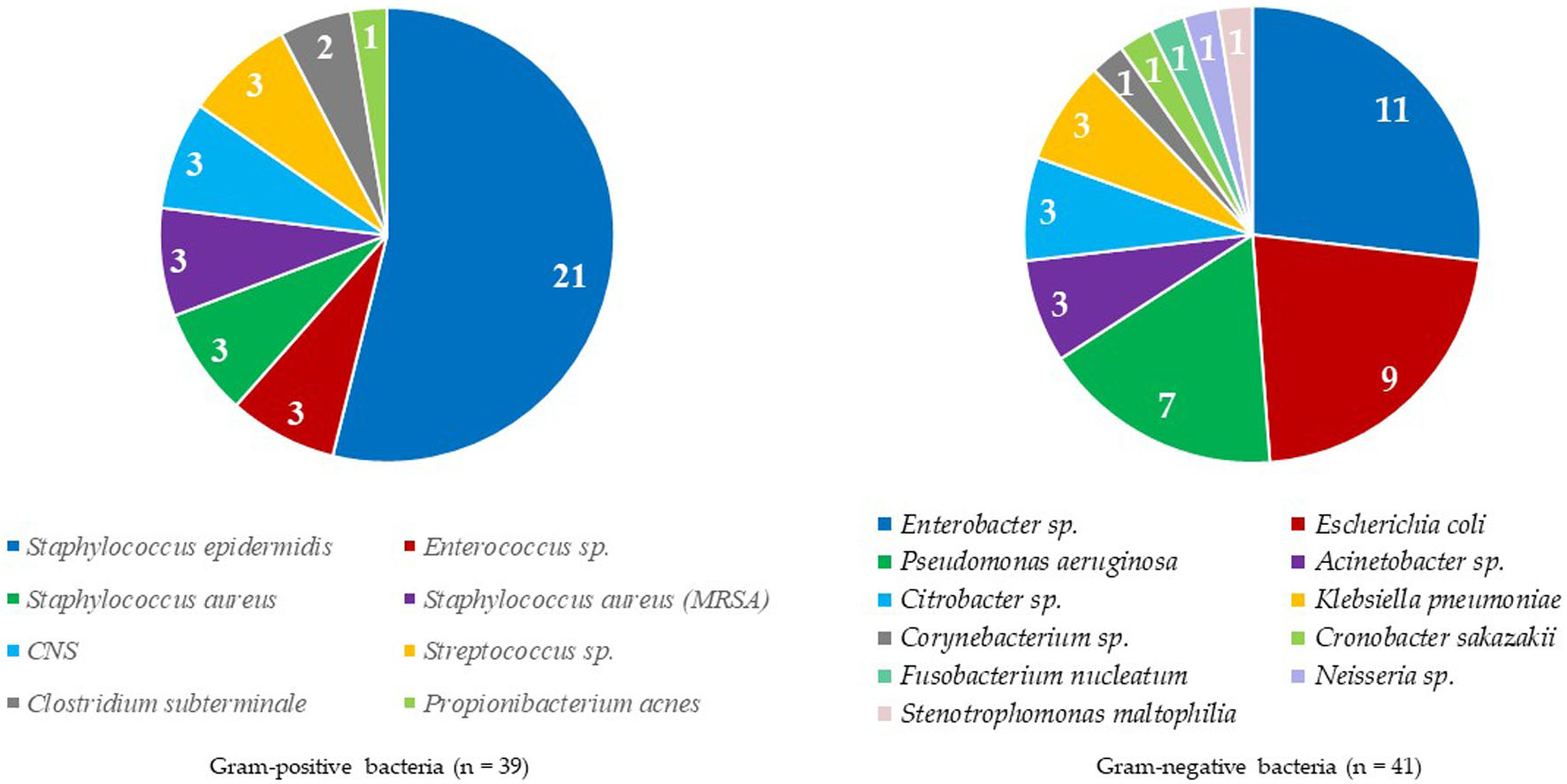 Click for large image | Figure 2. All detected bacteria in inflammatory bowel disease patients with bloodstream infections. |
Table 1 provides a summary of the clinical backgrounds of the patients. There were no significant differences in the median age, BMI, or prevalence of diabetes between the two groups. Immunosuppressive drug use was higher in the CD group than in the UC group (57.4% vs. 11.1%, respectively; P = 0.00003). The hospital stay length was significantly longer in the UC group (median 15 days; 6.0 - 68.0 days) than in the CD group (median 9 days; 2 - 24.3 days) (P = 0.045). There was no statistical correlation between immunosuppressant use and length of hospital stay (immunosuppressant user: 9.5 days (2.3 - 30.3) vs. non-users: 15 days (1 - 30.0), P = 0.446).
 Click to view | Table 1. Comparisons of Clinical Characteristics Between CD and UC Patients and Infection Focus in Patients With BSI |
There was no difference in the detection rates between the two groups for 16 bacterial species, including Staphylococcus aureus. The detection rate of gram-negative bacilli was significantly higher in the UC group (Table 2). The detection rates of Pseudomonas aeruginosa (P. aeruginosa) and Klebsiella pneumoniae (K. pneumoniae) were higher in the UC than the CD patients (18.5% vs. 2.9%, P = 0.021; 11.1% vs. 0%, P = 0.019, respectively).
Click to view | Table 2. Percentage of Detected Bacteria in Patients With CD and UC |
| Discussion | ▴Top |
In this study, we found significant differences in the types of bacteria detected in CD and UC patients. Due to the nature of the condition, IBD patients often have a catheter inserted into their central artery and an additional intestinal fistula, such as a stoma [9]. This might explain why S. epidermidis, which lives in the epidermis, was detected as the most common causative bacterium among the gram-positive bacteria. Similarly, Enterobacter spp. and E. coli may have been found in greater numbers among the gram-negative bacteria because they are found in greater numbers in the intestinal flora. When both groups were considered as a single group of IBD patients, it became clear that their epidemiology was similar to that of the causative microorganisms in ordinary bacteremia patients [10]. Thus, we concluded that the major BSI-causing organisms did not differ in IBD and non-IBD patients.
The detection rates for K. pneumoniae and P. aeruginosa were significantly higher in the UC group compared to the CD group. The high detection rate of K. pneumoniae in the UC group was probably because the fine structural damage in the tight junctions between mucosal epithelial cells increased the detection rate of K. pneumoniae. Ultrastructure disorders are attributed to tight junctions and cytokines that affect intestinal permeability [1], which allows bacterial translocation and, in severe cases, bacterial invasion to occur due to mucosal defense dysfunction [1]. In such cases, the intestinal flora (e.g., K. pneumoniae) permeates the intestinal tract with bacteria, which can cause bloodstream disease. Additionally, UC typically has reduced mucus barrier function due to embryonic cell miniaturization and decreased mucin production [11]. These features are usually perceived as inflammatory changes since changes in goblet cells can also occur in infectious enteritis; however, a slight decrease in mucus barrier function is also observed in the proximal intestinal tract in patients with distal UC, suggesting that it is an early predisposition that precedes histological inflammation [12]. Thus, we concluded that the high K. pneumoniae detection rate in the UC group could have been due to intestinal flora invasion of the blood due to bacterial translocation.
The detection rate of P. aeruginosa was also significantly higher in the UC patient group. Since P. aeruginosa is not a common intestinal flora [13], it is unlikely that bacterial translocation occurred in the same manner as K. pneumoniae. The significantly longer hospital stay lengths found in the UC group compared to the CD group could have allowed for the significant increase in P. aeruginosa in the UC group [14]. Prolonged hospitalization and the use of immunosuppressants are risk factors for BSI [15, 16]. Patients with P. aeruginosa had significantly longer median hospital stay length in comparison to those with other bacteria (40 (13.5 - 237.5) vs. 10 (0.75 - 28.0), P = 0.0263), but similar trend was not observed in patients with K. pneumoniae. In fact, the use of immunosuppressants can cause clinical problems with attenuated P. aeruginosa strains. In this study, the use of immunosuppressants was significantly higher in CD patients, but the hospital stay length was significantly higher in the UC patients. In addition, there was no correlation between immunosuppressant use and length of hospital stay, and no significant difference in the detection rate of bacteria between patients with and without the use of immunosuppressant (Supplementary Material 1, www.jocmr.org). These results could explain why the UC patients had significantly more P. aeruginosa than the CD patients. Thus, P. aeruginosa-derived BSI in CD and UC patients may depend on hospital stay length. Taken together, our findings indicate that IBD patients may require different treatment strategies at BSI onset depending on the type of IBD they have (CD or UC). In particular, UC patients may need therapies that target P. aeruginosa and K. pneumoniae at BSI onset.
This study had a few limitations. First, this was a pilot study retrospectively conducted in a single Japanese hospital with a relatively small study cohort; therefore, our findings may not be generalized to other hospitals or countries. Second, this study investigated only IBD patients with bacteremia and did not examine any clinical and/or microbiological factors related to bacteremia. A comparative study using a control group using statistical methods such as propensity score matching is needed to clarify the factors associated with bacteremia in IBD patients. Third, although blood culture has been the most common method for diagnosis of bloodstream pathogens, it is being supplanted with more advanced methods, such as molecular tests that can reduce the turnaround time from several days to a few hours [17]. Unfortunately, we have not yet been able to apply such technology to clinical practice, but we plan to consider it and compare these methods in terms of sensitivity and specificity for bacterial detection in the future.
This study showed that K. pneumoniae and P. aeruginosa had higher abundance in UC patients at the onset of BSI. Furthermore, long-term hospitalized patients with UC required antimicrobial therapy against K. pneumoniae and P. aeruginosa.
| Supplementary Material | ▴Top |
Suppl 1. Percentage of Detected Bacteria in the Use of Immunosuppressants.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
The authors declare that they have no competing interests.
Informed Consent
Not applicable.
Author Contributions
KM, MM, and OI contributed to the concept and design of the study. KM, MM, KM, and YK conducted the study. KM, AN, TN, and DH were involved with data analysis and interpretation of the results. KM and MM drafted the manuscript. KM, DH, and OI supervised the entire project and reviewed the manuscript. All the authors approved the final version of the manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Fakhoury M, Negrulj R, Mooranian A, Al-Salami H. Inflammatory bowel disease: clinical aspects and treatments. J Inflamm Res. 2014;7:113-120.
doi pubmed pmc - Frank DN, St Amand AL, Feldman RA, Boedeker EC, Harpaz N, Pace NR. Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases. Proc Natl Acad Sci U S A. 2007;104(34):13780-13785.
doi pubmed pmc - Wehkamp J, Schmid M, Fellermann K, Stange EF. Defensin deficiency, intestinal microbes, and the clinical phenotypes of Crohn's disease. J Leukoc Biol. 2005;77(4):460-465.
doi pubmed - Ley RE, Peterson DA, Gordon JI. Ecological and evolutionary forces shaping microbial diversity in the human intestine. Cell. 2006;124(4):837-848.
doi pubmed - Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, Sargent M, Gill SR, et al. Diversity of the human intestinal microbial flora. Science. 2005;308(5728):1635-1638.
doi pubmed pmc - Matsuoka K, Kanai T. The gut microbiota and inflammatory bowel disease. Semin Immunopathol. 2015;37(1):47-55.
doi pubmed pmc - Al-Hasan MN, Wilson JW, Lahr BD, Eckel-Passow JE, Baddour LM. Incidence of Pseudomonas aeruginosa bacteremia: a population-based study. Am J Med. 2008;121(8):702-708.
doi pubmed pmc - Ministry of Health, Labour and Welfare. Japan Nosocomial Infections Surveillance. https://janis.mhlw.go.jp/report/kensa.htm. Accessed Oct 3, 2022.
- Shibata W, Sohara M, Wu R, Kobayashi K, Yagi S, Yaguchi K, Iizuka Y, et al. Incidence and outcomes of central venous catheter-related blood stream infection in patients with inflammatory bowel disease in routine clinical practice setting. Inflamm Bowel Dis. 2017;23(11):2042-2047.
doi pubmed - Nakada Y, Fujiwara H, Kaminada N, Takane H, Chikumi H. Blood culture-positive episodes in a tertiary university hospital in Japan. Jpn J Environ Infect. 2016;31:107-112.
- Tytgat KM, van der Wal JW, Einerhand AW, Buller HA, Dekker J. Quantitative analysis of MUC2 synthesis in ulcerative colitis. Biochem Biophys Res Commun. 1996;224(2):397-405.
doi pubmed - Wlodarska M, Thaiss CA, Nowarski R, Henao-Mejia J, Zhang JP, Brown EM, Frankel G, et al. NLRP6 inflammasome orchestrates the colonic host-microbial interface by regulating goblet cell mucus secretion. Cell. 2014;156(5):1045-1059.
doi pubmed pmc - Ramphal R. Infections due to Pseudomonas, Burkholderia, and Stenotrophominas species. In: Jameson JL, Fauci AS, Kasper DL, et al., editors. Harrison’s principles of internal medicine, 20th ed. McGraw-Hill, New York, NY, USA. 2018; p. 1167-1173.
- Porco FV, Visconte EB. Pseudomonas aeruginosa as a cause of infectious diarrhea successfully treated with oral ciprofloxacin. Ann Pharmacother. 1995;29(11):1122-1123.
doi pubmed - Kollef MH, Zilberberg MD, Shorr AF, Vo L, Schein J, Micek ST, Kim M. Epidemiology, microbiology and outcomes of healthcare-associated and community-acquired bacteremia: a multicenter cohort study. J Infect. 2011;62(2):130-135.
doi pubmed - Delle Rose D, Pezzotti P, Fontana C, Altieri A, Minelli S, Mariotti B, Cerretti R, et al. An in-depth analysis of nosocomial bloodstream infections due to Gram-negative bacilli: clinical features, microbiological characteristics and predictors of mortality in a 1 year, prospective study in a large tertiary care Italian hospital. Infect Dis (Lond). 2019;51(1):12-22.
doi pubmed - Dunbar SA, Gardner C, Das S. Diagnosis and management of bloodstream infections with rapid, multiplexed molecular assays. Front Cell Infect Microbiol. 2022;12:859935.
doi pubmed pmc
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.