

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://www.jocmr.org |
Original Article
Volume 14, Number 11, November 2022, pages 466-473

Effect of Omega-3 Polyunsaturated Fatty Acids Intake on Eosinophil Airway Inflammation in University Athletes
Tomoko Imaia, d, Yutaro Takadab, Koichi Watanabec
aCenter for Genera Education, Aichi Institute of Technology, Toyota 470-0392, Japan
bUniversity of Hawai’I at Manoa Athletic Department, Honolulu, HI 96822, Japan
cFaculty of Health and Sport Sciences, University of Tsukuba, Tsukuba, Ibaraki 305-8577, Japan
dCorresponding Author: Tomoko Imai, Center for General Education, Aichi Institute of Technology, Toyota 470-0392, Japan
Manuscript submitted September 13, 2022, accepted November 7, 2022, published online November 29, 2022
Short title: n-3 PUFA on Eosinophil Airway Inflammation
doi: https://doi.org/10.14740/jocmr4825
| Abstract | ▴Top |
Background: Though athletes have a high risk of respiratory disorders, effective prevention has not yet to be identified. Omega-3 (n-3) polyunsaturated fatty acids (PUFA) have some practical anti-inflammatory effects in allergy, and therefore may reduce airway inflammation in athletes. This study aimed to assess whether n-3 PUFA intake affects airway inflammation in university athletes.
Methods: Twenty-three males were divided into three groups: 1) the eosinophilic airway inflammation group (I_PUFA group; fractional exhaled nitric oxide (FeNO ≥ 25 ppb, n = 10); 2) the non-eosinophilic airway inflammation group (N_PUFA group; FeNO < 25 ppb, exhaled carbon dioxide (eCO) ≥ 3.6 ppm, n = 5); and 3) the control group (FeNO < 25 ppb, eCO < 3.6 ppm, n = 8). Participants took supplements containing 260 mg of docosapentaenoic acid and 600 mg of eicosapentaenoic acid (EPA) daily for 3 weeks. Baseline measurements of FeNO, respiratory impedance, respiratory function, dietary intake (food frequency questionnaires), and blood tests were performed. FeNO and respiratory impedance were measured weekly, and the rest were measured after 3 weeks.
Results: There was a significant decrease in FeNO levels from baseline at 2 and 3 weeks in the I_PUFA group (54.7 ± 8.5 ppb vs. 45.1 ± 9.1 and 45.4 ± 7.7 ppb; mean ± standard error (SE), P < 0.05). After 3 weeks, FeNO levels remained unchanged in the N_PUFA and control groups, and respiratory impedance and function remained unchanged in all groups. Blood EPA levels significantly increased in the I_PUFA and N_PUFA groups (I_PUFA, 27.7 ± 16.9 vs. 52.1 ± 12.3 µg/mL; N_PUFA, 20.8 ± 8.7 vs. 70.4 ± 36.1 µg/mL; mean ± standard deviation (SD), P < 0.05). No changes were observed in dietary intake over the 3 weeks.
Conclusions: n-3 PUFA supplementation for 3 weeks reduced airway inflammation in athletes with FeNO levels ≥ 25 ppb.
Keywords: Polyunsaturated fatty acids; Airway inflammation; Athletes
| Introduction | ▴Top |
Athletes have a high risk of respiratory disorders [1, 2] because a high ventilation volume during exercise damages the airway endothelial cells by mechanical stress and dehydration of the surface area [3, 4]. However, athletes need to regularly participate in high-intensity training to improve their daily performance. Therefore, their airway endothelial cells may not have time to sufficiently recover before the following training session, putting them at risk of developing airway inflammation [4, 5]. Chronic mechanical stress on the airway can result in worse damage and lead to exercise-induced asthma and bronchial hyperresponsiveness [4, 6]. However, to date, there is no clear evidence regarding strategies to improve and prevent respiratory disorders in athletes.
Omega-3 (n-3) polyunsaturated fatty acids (PUFA), eicosatetraenoic acid (EPA), and docosahexaenoic acid (DHA) in fish oil have anti-inflammatory and protective effects against inflammatory diseases [7-9]. Mickleborough et al showed that intake of n-3 PUFA for 3 weeks improved postexercise pulmonary function and significantly suppressed the proinflammatory eicosanoid and cytokine levels in elite athletes with exercise-induced bronchoconstriction (EIB) [9] and asthma [10]. Regular intake of n-3 PUFA increases anti-oxidate function by inhibiting the arachidonic acid (AA) cascade of omega-6 derived from pre-inflammation, such as NF-κB and inflammatory cytokines [11, 12]. It has also been shown to improve physical function and prevent infection in athletes, and increase muscle protein synthesis, muscle strength, and neuromuscular function [12-14]. Moreover, n-3 PUFA intake improves cardiovascular function response during exercise [15, 16], and may increase the potential protective role of various biological defenses and support the improvement of physical function in athletes [13-17].
However, the effect of n-3 PUFA intake on airway inflammation in athletes has not been sufficiently investigated. An intake of fish oil could inhibit airway inflammation in athletes, thus playing a role in preventing the development of EIB. Furthermore, athletes’ respiratory disorders are affected by sports type, environment, and individual factors [2, 18]; hence, it may be necessary to verify the effectiveness of n-3 PUFA supplements in preventing the effects of airway inflammation in athletes.
Therefore, we examined whether n-3 PUFA supplement intake inhibits airway inflammation response in American football players. To assess airway inflammation, we measured fractional exhaled nitric oxide (FeNO), FeNO ≥ 25 ppb is defined an eosinophilic acid marker [19], and exhaled carbon dioxide (eCO). While FeNO is a major indicator of airway inflammation, eCO has also been reported as an index of airway diseases such as asthma; therefore, we used a combination of both measures for a robust assessment [20]. In addition, we used oscillation as a non-load method, and respiratory impedance and oscillation methods to assess whole respiratory function with non-effort dependent for a short time [21]. These assessment methods are not stressful for the athlete and can measure the whole respiratory impedance. Thus, this study aimed to assess, using FeNO whether intake of n-3 PUFA supplements affects eosinophil airway inflammation in university athletes.
| Materials and Methods | ▴Top |
Participants
This study enrolled 24 male university American football players who competed at a national level and trained 6 days a week (mean age, height, and weight: 20 ± 1.6 years, 172.8 ± 5.7 cm, and 79 ± 0.5 kg, respectively). One participant had a history of asthma. All participants were non-smokers and not taking medications. All participants took protein supplements.
This study was conducted following the principles outlined in the Declaration of Helsinki. It was approved by the Ethics Committee of Research and Aichi Institute of Technology (approval number 2017-1). All participants provided written informed consent before participating in the study.
n-3 PUFA supplements
Participants were given a commercially available drink-type supplement containing fish oil (Nissui imark S, Nissui Inc., Japan). The supplement contained 860 mg of n-3 PUFA, of which 260 mg was DHA and 600 mg was EPA. Participants were instructed to take one bottle daily (according to the dosage recommended by the manufacturer) for 3 weeks. In addition, the participants were instructed not to change their diet over the 3 weeks and were followed up weekly regarding whether they were consuming the daily supplements.
Experimental protocol
Participants’ physical characteristics, FeNO and eCO levels, respiratory impedance, and bloods were measured four times in the measurement room. Respiratory function and dietary habits (via food frequency questionnaires (FFQ)) were assessed on the first and fourth visit. Blood samples were collected after respiratory measurements on the same day. Participants fasted from 9 pm on the day prior to measurement and refrained from high-intensity exercise, alcohol, and caffeine. On the measurement day, participants were allowed to consume water only. We conducted questionnaires using Google forms (free software) to obtain medical history regarding asthma and medication intake, including supplement intake. Measurements were taken between 6 am and 8 am. Respiratory function was assessed after measuring FeNO, eCO, and respiratory impedance.
After obtaining baseline measurements, the participants were divided into two groups as follows: the eosinophilic airway inflammation group (I_PUFA group; FeNO ≥ 25 ppb, n = 10) and the non-eosinophil airway inflammation group (N_PUFA group; FeNO < 25 ppb, n = 13). In addition, a third control group (no PUFA intake group; n = 8) was established from the N_PUFA group. Participants for the control group were selected based on eCO levels of < 3.6 ppm, which have been indicated as healthy levels by previous studies [22]. Increased eCO levels have been reported in some respiratory disorders [23].
n-3 PUFA supplements were distributed once a week on measuring day. We confirmed via a record sheet whether or not participants took the supplement every day during their weekly visits to the measurement room.
Physical characteristics, nitric oxide, spirometry, and respiratory impedance
Body weight was measured using health meters (UC411PBT-C, A&D Co. Ltd, Tokyo, Japan). FeNO was measured using a portable NIOX Vero (Aerocrine AB, Stockholm, Sweden), according to European Respiratory Society and American Thoracic Society recommendations, and eCO was measured using a portable CARBOLYZER II (Taiyo Inc. Osaka, Japan). FeNO and eCO levels were assessed before spirometry and respiratory impedance, as per established guidelines. Pulmonary function was determined using HI-801 spirometry (Chest M.I., Tokyo, Japan). We performed the standard measures of pulmonary function, including forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), and peak expiratory flow (PEF) at baseline and 3 weeks. The predicted value and forced expiratory volume in 1 s for a Japanese population were calculated using the formula proposed by the Japanese Respiratory Society. All tests were performed according to the methods described in the Japanese Respiratory Society guidelines.
Respiratory impedance was assessed via forced oscillation technique (FOT) using the Most Graph-01 (Chest M.I., Tokyo, Japan). Participants sat in a neutral position and measurements were taken while using a nose clip. The parameters used were resistance at 5 Hz (R5), resistance at 20 Hz (R20), reactance at 5 Hz (X5), and resonant frequency (Fres), where the reactance crossed zero and the elastic and inertial forces were equal in magnitude and opposite in direction. In addition, mouth pressure and flow signals were measured and used to calculate respiratory impedance via computer algorithms [24].
Short version semi-quantitative FFQ
We used the short version semi-quantitative FFQ to assess the participants’ dietary habits. The short version of the FFQ is composed of 94 food types classified into 12 categories. Participants completed the FFQ twice, at baseline and 3 weeks. The food consumed was calculated according to the amount consumed daily, weekly, or monthly. The total energy, lipid, protein, and carbohydrate intakes at baseline and 3 weeks were compared. FFQ data were analyzed using Education Software Co., Ltd (Tokyo, Japan).
Statistical analyses
Data were expressed as mean ± standard deviation (SD) or mean ± standard error (SE). Variances across the groups at different time points were evaluated using analysis of variance for repeated measurements. In addition, a post hoc test (Fisher’s least significant difference (LSD) test) was used to determine specific significant differences between groups at different time points, when a significant F value was observed. Statistical significance was set a priori at P < 0.05. Statistical analyses were performed using STATISTICA version 10.
| Results | ▴Top |
The data of one participant were excluded from the analysis due to incomplete measurements. The physical characteristics of the three groups at baseline and the pulmonary function test data are shown in Table 1. Pulmonary function was not significantly changed.
 Click to view | Table 1. Respiratory Function at Baseline and After 3 Weeks |
Figure 1 shows the changes in FeNO over the 3 weeks. FeNO were significantly higher in the I_PUFA group than in the N_PUFA and control groups at baseline. FeNO in the I_PUFA group at 2 and 3 weeks were significantly decreased compared with that at baseline and 1 week. FeNO in the N_PUFA and control groups did not change over the 3 weeks. Blood eosinophil did not significantly differ between the groups for 3 weeks (Table 2). eCO were significantly decreased at 2 and 3 weeks in the I_PUFA and N_PUFA groups while they remained unchanged in the control group.
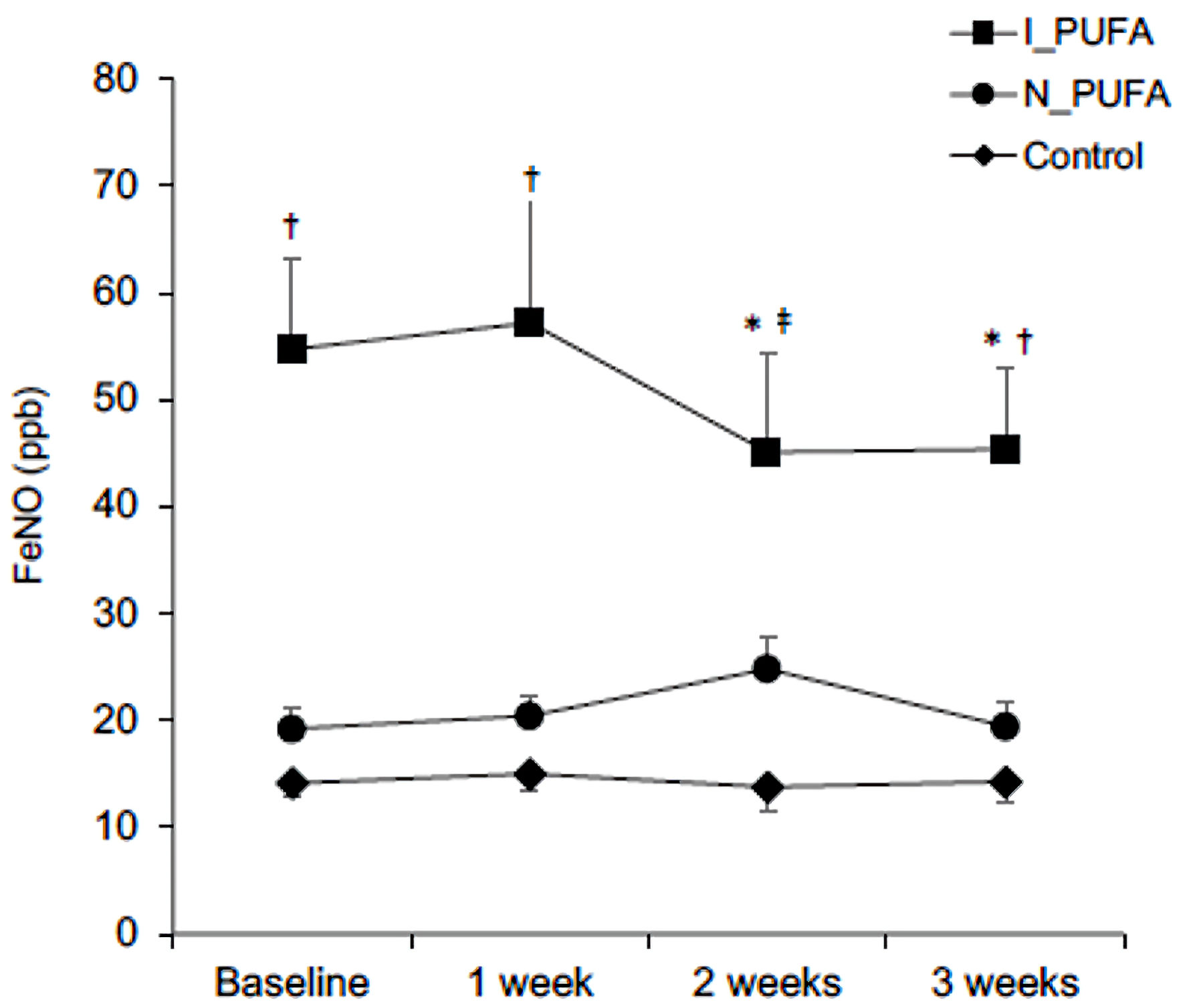 Click for large image | Figure 1. Comparison of FeNO levels at baseline and after 1, 2, and 3 weeks of PUFA supplementation between the three groups. Error bars represent standard deviations. *P < 0.05 vs. baseline and 1 week. †P<0.05 vs. N_PUFA and control. ‡P < 0.05 vs. control. PUFA: polyunsaturated fatty acids; I: airway inflammation; N: non-airway inflammation; I_PUFA: intake of PUFA and FeNO ≥ 25 ppb; N_PUFA: intake of PUFA and FENO < 25 ppb and eCO ≥ 3.6 ppm; FeNO: fractional exhaled nitric oxide. |
Click to view | Table 2. Changes in eCO and Blood Eosinophils Levels Over 3 Weeks |
Table 3 shows respiratory impedance measurements for the three groups. Respiratory impedance could not be assessed in two participants from the N_PUFA group. FOT was assessed in the I_PUFA and control groups. No significant differences were observed in resistance and impedance measurements between the I_PUFA and control groups.
Click to view | Table 3. Changes in Respiratory Impedance Markers Over 3 Weeks |
Table 4 shows the FFQ results. Total energy, lipid, protein, and carbohydrate intake levels did not change over the 3 weeks. Blood n-3 PUFA measurements showed significant increases in EPA and EPA/AA levels in the I_PUFA and N_PUFA groups after 3 weeks but no changes were observed in the control group (Table 5).
Click to view | Table 4. Dietary Intake as Assessed by the Food Frequency Questionnaire at Baseline and 3 Weeks |
Click to view | Table 5. Changes in Blood n-3 PUFA Over 3 Weeks |
| Discussion | ▴Top |
In this study, we investigated the effect of taking n-3 PUFA supplements on airway inflammation in university athletes. Daily n-3 PUFA intake for 3 weeks significantly decreased FeNO levels in the I_PUFA group but not in the N-PUFA group, which indicates that n-3 PUFA intake may be effective in athletes with existing eosinophil airway inflammation. In addition, eCO levels significantly decreased in both the I_PUFA and N_PUFA groups after 2 weeks. In contrast, respiratory impedance and resistance did not change in the I_PUFA and control groups, and blood eosinophils did not change over the 3 weeks.
The inspiration of cool and/or dry air and high ventilation rates during exercise can dehydrate the airway surface [6]. This transient dehydration causes an increase in airway liquid osmolarity. As a result, the surface of airway cells leaks out, activating histamine, neuro peptides, and arachidonic acid metabolites, such as cysteinyl-leukotrienes and prostaglandins [3, 4]. These eicosanoids cause bronchial smooth muscle contraction and subsequent airway obstruction [3]. Previous studies reported that n-3 PUFA might reduce the generation of inflammatory leukotrienes and prostaglandins [25, 26]. Therefore, n-3 PUFA may interfere with early inflammatory signal transduction processes [27]. In this study, FeNO levels, an index of eosinophil airway inflammation, significantly decreased in the I_PUFA group after 2 weeks of n-3 PUFA intake. However, respiratory function and respiratory impedance did not change in all groups, suggesting that the effectiveness of n-3 PUFA might be limited. However, this absence of change in airway state may still have significant meaning for athletes because they are exposed to various stresses and respiratory risk factors from training. Therefore, the prevention of respiratory function impairment is necessary in athletes who train almost daily, and n-3 PUFA may play a role by preventing airway inflammation.
Mickleborough et al showed that the greater the EPA content of a fish oil formulation, the greater the eicosanoid and cytokine reduction in elite athletes and patients with asthma [9, 10]. FeNO is synthesized from L-arginine by inducible nitric oxide synthase (iNOS) enzymes, in response to inflammatory cytokines. In addition, the expression of iNOS is controlled by mast cells, eosinophils, and the expression of iNOS is enhanced via STAT-6 from interleukin (IL)-4/13 [28]. On the other hand, sufficient intake of n-3 PUFA may inhibit the production of inflammatory cytokines and iNOS activity. Therefore, although blood eosinophil levels may not change, FeNO levels may be decreased through the inhibition of iNOS production [29]. However, no change in blood eosinophil may also indicate that FeNO levels increase again when n-3 PUFA intake is stopped. Thus, to reduce eosinophil levels, long-term n-3 PUFA intake or dietary modification would be necessary.
Eosinophils have been recently reported to not only induce the proinflammatory response but also play a role in the pro-resolving response [30]. Sawane et al suggested that eosinophil functions are determined by the surrounding lipid environment in mice [31]. In addition, an increase in EPA and DHA levels have been shown to decrease the production of inflammatory mediators by macrophages and granulocytes at the site of inflammation [32]. Furthermore, the endogenous lipid metabolites of n-3 PUFA are specialized pro-resolving mediators involved in promoting the resolution of inflammation. Hence, although blood eosinophil did not change over the 3 weeks in our study, the change in the lipid environment of the body may have contributed to the inhibition of airway inflammation. Meanwhile, FeNO did not change in the N_PUFA group after 3 weeks. Moreira et al [33] previously reported that short-term dietary supplementation with n-3 PUFA in women with stable asthma was not associated with statistically significant changes in FeNO; however, their participants’ FeNO levels were not very high level (FeNO < 50 ppb). A higher FeNO level might be more strongly affected by n-3 PUFA intake.
Levels of eCO were significantly decreased in both the I_PUFA and N_PUFA groups. Exercise training and environmental factors load the airway and induce airway inflammation in athletes [1]. This airway inflammation may not only be caused by eosinophils but basophils and oxidative stress also [3]. Endogenous CO is produced through heme oxygenase 1 (HO-1) degradation to heme iron and biliverdin and the exposure of airway epithelial cells to oxidative stress increases HO-1 production [34]. A decrease in eCO may reflect the effect of n-3 PUFA in reducing oxidative stress of the airway. Supplementation of n-3 PUFA is known to reduce systematic oxidative stress [35]. HO-1 also has antioxidant functions and protects against tissue injury and airway inflammation [36].
Traditionally, Japanese people are more accustomed to eating fish than people from Europe and the USA. However, young Japanese people tend to prefer a western-style diet to traditional Japanese diets [37]. Low EPA/AA intake increases the risk of cardiovascular events, chronic inflammation, and impaired glucose tolerance [12]. In addition, EPA/AA balance is associated with maintaining immune function and preventing allergies. Fish oil supplementation has positive implications in healthy individuals with dietary-induced airway inflammation [38]. In this study, while airway inflammation makers in the N_PUFA group did not change, the increase in EPA/AA might be important for preventing metabolic disorders in the future [39].
We investigated the participants’ respiratory impedance using the FOT. The FOT can easily measure respiratory parameters in a short amount of time and is noninvasive [40]. In addition, it is a common for athletes to regularly measure their respiratory resistance to screen for and prevent respiratory disorders, and the FOT can assess whole respiratory function in detail.
n-3 PUFA supplementation did not change respiratory impedance in both the I_PUFA and N_PUFA groups after 3 weeks. The I_PUFA group had eosinophil airway inflammation but did not have high respiratory impedance compared with the control group. The development of chronic airway inflammation induces asthma. In this study, respiratory impedance did not change pre- and post n-3 PUFA supplementation. However, if airway inflammation was severe, follow-up would have been required.
Pulmonary function did not change in all groups. Previous studies have reported increases in pulmonary function after n-3 PUFA supplement intake in asthmatic athletes [41]. Although the I_PUFA group had high FeNO levels, pulmonary function was not reduced before intake of the supplement, and they were not diagnosed with asthma. Therefore, pulmonary function may not be significantly changed by n-3 PUFA intake.
The factors of airway inflammation are complex in athletes, thus identifying one specific cause of inflammation in this population is impossible. n-3 PUFA intake can inhibit inflammation in general; therefore, it might be an effective tool to prevent the development of EIB, asthma, and airway inflammation in athletes. However, n-3 PUFA supplements are expensive and, in some cases, might increase the risk of doping. It may also be necessary to review dietary intakes before increasing intakes of n-3 PUFA.
All participants took protein supplements. Protein supplements are widely recommended to athletes to maintain physical condition and help gain muscle mass. However, the impact of long-term, high intake protein supplementation in athletes are not known [42]. Protein supplements might induce allergies because most include casein protein, a common allergen. Moreno-Perez et al [42] also showed that a slight increase in protein intake in athletes decreases health-promoting bacteria in the microbiota. The gut microbiota is an important factor in the onset of allergic disease. On the other hand, in children, IgE significantly decreased following whey supplementation [43]. Thus, the influence of long-term supplementation requires further investigation.
We chose a drink-type supplement as it is easier to swallow compared with the capsule type. The dose of n-3 PUFA in this study (0.87 g/day) was lower than previous studies [44]. However, the dose of n-3 PUFA required to improve respiratory disorders has not been determined. Low-dose allergen tests showed that an n-3 PUFA-enriched fat blend (0.69 g/day) was able to reduce bronchial inflammation [26]. Considering the high cost of n-3 PUFA supplements, long-term high-dose supplementation may not be feasible, particularly for young athletes [45]. Thus, it may be necessary to consider the minimum dose and effect of n-3 PUFA.
Limitations
This study has some limitations. First, the number of participants was small. Different training environments and exercise types can affect the extent of airway epithelial damage. Therefore, to reduce confounding factors when investigating the effects of n-3 PUFA supplementation, it is necessary to control such variances in participant characteristics. To this end, participants were recruited from the same sports team. Hence, the sample size in this study was small. The statistical significance of our results may be limited by the small sample size and wide variability in airway inflammation. Nevertheless, to mitigate this, we used two indices to assess airway inflammation and included a control group.
Second, we did not use a placebo supplement drink for the control group. However, we compared the supplement group and the control group. Third, we confirmed changes in blood EPA and DHA levels by assessing the difference between the supplement group and the control group. As a result, we found that airway inflammation was reduced in the I_PUFA group but not in the N_PUFA group. Finally, we could not clarify the effect of preventing airway inflammation because airway inflammation in the N_PUFA group was not significantly different from that in the control group. We could get the results of decreasing the high FeNO level, over 50 ppb.
Further studies are required to elucidate the effectiveness of n-3 PUFA supplements in preventing exercised-induced asthma and airway inflammation in athletes.
Conclusions
A daily intake of n-3 PUFA supplements (0.87 g/day) for 3 weeks reduced airway inflammation in athletes with baseline FeNO levels ≥ 25 ppb. However further studies with larger sample sizes are required to validate this result.
Acknowledgments
We would like to thank the peer reviewers and editors for their opinions and suggestions.
Financial Disclosure
This work was supported in part by the Japan Society for the Promotion of Science Grants-in-Aid for Scientific Research (KAKENHI) Grant Number 20K11400.
Conflict of Interest
The authors have no potential conflicts of interest to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
TI and KW designed the experiments; TI and YT performed the experiments; TI analyzed the data and wrote the paper.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
n-3: omega-3; PUFA: polyunsaturated fatty acid; I_PUFA: intake of PUFA and FeNO ≥ 25 ppb; N_PUFA: intake of PUFA and FENO < 25 ppb and eCO ≥ 3.6 ppm; FeNO: fractional exhaled nitric oxide; eCO: exhaled carbon dioxide; FFQ: food frequency questionnaire; EPA: eicosatetraenoic acid; DHA: docosahexaenoic acid; EIB: exercise-induced bronchoconstriction; AA: arachidonic acid; FOT: forced oscillation technique; FVC: forced vital capacity; FEV1: forced expiratory volume in the first second; PEF: peak expiratory flow; R5: resistance at 5 Hz; R20: resistance at 20 Hz; X5: reactance at 5 Hz; Fres: resonant frequency; HO-1: heme oxygenase 1
| References | ▴Top |
- Kippelen P, Fitch KD, Anderson SD, Bougault V, Boulet LP, Rundell KW, Sue-Chu M, et al. Respiratory health of elite athletes - preventing airway injury: a critical review. Br J Sports Med. 2012;46(7):471-476.
doi pubmed - Haahtela T, Malmberg P, Moreira A. Mechanisms of asthma in Olympic athletes—practical implications. Allergy. 2008;63(6):685-694.
doi pubmed - Rundell KW, Jenkinson DM. Exercise-induced bronchospasm in the elite athlete. Sports Med. 2002;32(9):583-600.
doi pubmed - Anderson SD, Kippelen P. Airway injury as a mechanism for exercise-induced bronchoconstriction in elite athletes. J Allergy Clin Immunol. 2008;122(2):225-235.
doi pubmed - Kippelen P, Anderson SD. Airway injury during high-level exercise. Br J Sports Med. 2012;46(6):385-390.
doi pubmed - Anderson SD, Holzer K. Exercise-induced asthma: is it the right diagnosis in elite athletes? J Allergy Clin Immunol. 2000;106(3):419-428.
doi pubmed - Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64(1):27-34.
doi pubmed - Mickleborough TD, Lindley MR, Montgomery GS. Effect of fish oil-derived omega-3 polyunsaturated Fatty Acid supplementation on exercise-induced bronchoconstriction and immune function in athletes. Phys Sportsmed. 2008;36(1):11-17.
doi pubmed - Mickleborough TD, Murray RL, Ionescu AA, Lindley MR. Fish oil supplementation reduces severity of exercise-induced bronchoconstriction in elite athletes. Am J Respir Crit Care Med. 2003;168(10):1181-1189.
doi pubmed - Mickleborough TD, Lindley MR, Ionescu AA, Fly AD. Protective effect of fish oil supplementation on exercise-induced bronchoconstriction in asthma. Chest. 2006;129(1):39-49.
doi pubmed - Kumar A, Mastana SS, Lindley MR. n-3 Fatty acids and asthma. Nutr Res Rev. 2016;29(1):1-16.
doi pubmed - Jeromson S, Gallagher IJ, Galloway SD, Hamilton DL. Omega-3 Fatty Acids and Skeletal Muscle Health. Mar Drugs. 2015;13(11):6977-7004.
doi pubmed - Guzman JF, Esteve H, Pablos C, Pablos A, Blasco C, Villegas JA. DHA- Rich Fish Oil Improves Complex Reaction Time in Female Elite Soccer Players. J Sports Sci Med. 2011;10(2):301-305.
- Walser B, Stebbins CL. Omega-3 fatty acid supplementation enhances stroke volume and cardiac output during dynamic exercise. Eur J Appl Physiol. 2008;104(3):455-461.
doi pubmed - Buckley JD, Burgess S, Murphy KJ, Howe PR. DHA-rich fish oil lowers heart rate during submaximal exercise in elite Australian Rules footballers. J Sci Med Sport. 2009;12(4):503-507.
doi pubmed - Maughan RJ, Burke LM, Dvorak J, Larson-Meyer DE, Peeling P, Phillips SM, Rawson ES, et al. IOC consensus statement: dietary supplements and the high-performance athlete. Br J Sports Med. 2018;52(7):439-455.
doi pubmed - Simopoulos AP. Omega-3 fatty acids and athletics. Curr Sports Med Rep. 2007;6(4):230-236.
doi pubmed - Helenius I, Haahtela T. Allergy and asthma in elite summer sport athletes. J Allergy Clin Immunol. 2000;106(3):444-452.
doi pubmed - Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602-615.
doi pubmed - Zhang J, Yao X, Yu R, Bai J, Sun Y, Huang M, Adcock IM, et al. Exhaled carbon monoxide in asthmatics: a meta-analysis. Respir Res. 2010;11:50.
doi pubmed - Shirai T, Kurosawa H. Clinical Application of the Forced Oscillation Technique. Intern Med. 2016;55(6):559-566.
doi pubmed - Deveci SE, Deveci F, Acik Y, Ozan AT. The measurement of exhaled carbon monoxide in healthy smokers and non-smokers. Respir Med. 2004;98(6):551-556.
doi pubmed - Moscato U, Poscia A, Gargaruti R, Capelli G, Cavaliere F. Normal values of exhaled carbon monoxide in healthy subjects: comparison between two methods of assessment. BMC Pulm Med. 2014;14:204.
doi pubmed - Uchida A, Ito S, Suki B, Matsubara H, Hasegawa Y. Influence of cheek support on respiratory impedance measured by forced oscillation technique. Springerplus. 2013;2:342.
doi pubmed - Helenius I, Lumme A, Haahtela T. Asthma, airway inflammation and treatment in elite athletes. Sports Med. 2005;35(7):565-574.
doi pubmed - Schubert R, Kitz R, Beermann C, Rose MA, Lieb A, Sommerer PC, Moskovits J, et al. Effect of n-3 polyunsaturated fatty acids in asthma after low-dose allergen challenge. Int Arch Allergy Immunol. 2009;148(4):321-329.
doi pubmed - Mickleborough TD, Rundell KW. Dietary polyunsaturated fatty acids in asthma- and exercise-induced bronchoconstriction. Eur J Clin Nutr. 2005;59(12):1335-1346.
doi pubmed - Bjermer L, Alving K, Diamant Z, Magnussen H, Pavord I, Piacentini G, Price D, et al. Current evidence and future research needs for FeNO measurement in respiratory diseases. Respir Med. 2014;108(6):830-841.
doi pubmed - Liput KP, Lepczynski A, Ogluszka M, Nawrocka A, Polawska E, Grzesiak A, Slaska B, et al. Effects of Dietary n-3 and n-6 Polyunsaturated Fatty Acids in Inflammation and Cancerogenesis. Int J Mol Sci. 2021;22(13):6965.
doi pubmed - Jaudszus A, Gruen M, Watzl B, Ness C, Roth A, Lochner A, Barz D, et al. Evaluation of suppressive and pro-resolving effects of EPA and DHA in human primary monocytes and T-helper cells. J Lipid Res. 2013;54(4):923-935.
doi pubmed - Sawane K, Nagatake T, Hosomi K, Hirata SI, Adachi J, Abe Y, Isoyama J, et al. Dietary Omega-3 Fatty Acid Dampens Allergic Rhinitis via Eosinophilic Production of the Anti-Allergic Lipid Mediator 15-Hydroxyeicosapentaenoic Acid in Mice. Nutrients. 2019;11(12):2868.
doi pubmed - Stephensen CB. Fish oil and inflammatory disease: is asthma the next target for n-3 fatty acid supplements? Nutr Rev. 2004;62(12):486-489.
doi pubmed - Moreira A, Moreira P, Delgado L, Fonseca J, Teixeira V, Padrao P, Castel-Branco G. Pilot study of the effects of n-3 polyunsaturated fatty acids on exhaled nitric oxide in patients with stable asthma. J Investig Allergol Clin Immunol. 2007;17(5):309-313.
- Horvath I, Loukides S, Wodehouse T, Kharitonov SA, Cole PJ, Barnes PJ. Increased levels of exhaled carbon monoxide in bronchiectasis: a new marker of oxidative stress. Thorax. 1998;53(10):867-870.
doi pubmed - McClung JA, Levy L, Garcia V, Stec DE, Peterson SJ, Abraham NG. Heme-oxygenase and lipid mediators in obesity and associated cardiometabolic diseases: Therapeutic implications. Pharmacol Ther. 2022;231:107975.
doi pubmed - Lee IT, Luo SF, Lee CW, Wang SW, Lin CC, Chang CC, Chen YL, et al. Overexpression of HO-1 protects against TNF-alpha-mediated airway inflammation by down-regulation of TNFR1-dependent oxidative stress. Am J Pathol. 2009;175(2):519-532.
doi pubmed - Morinaka T, Wozniewicz M, Jeszka J, Bajerska J, Nowaczyk P, Sone Y. Westernization of dietary patterns among young Japanese and Polish females — a comparison study. Ann Agric Environ Med. 2013;20(1):122-130.
- Ade CJ, Rosenkranz SK, Harms CA. The effects of short-term fish oil supplementation on pulmonary function and airway inflammation following a high-fat meal. Eur J Appl Physiol. 2014;114(4):675-682.
doi pubmed - Yagi S, Aihara K, Fukuda D, Takashima A, Bando M, Hara T, Nishimoto S, et al. Reduced ratio of eicosapentaenoic acid and docosahexaenoic acid to arachidonic acid is associated with early onset of acute coronary syndrome. Nutr J. 2015;14:111.
doi pubmed - Nakano S, Nakahira J, Sawai T, Kuzukawa Y, Ishio J, Minami T. Perioperative evaluation of respiratory impedance using the forced oscillation technique: a prospective observational study. BMC Anesthesiol. 2016;16(1):32.
doi pubmed - Tartibian B, Maleki BH, Abbasi A. The effects of omega-3 supplementation on pulmonary function of young wrestlers during intensive training. J Sci Med Sport. 2010;13(2):281-286.
doi pubmed - Moreno-Perez D, Bressa C, Bailen M, Hamed-Bousdar S, Naclerio F, Carmona M, Perez M, et al. Effect of a protein supplement on the gut microbiota of endurance athletes: a randomized, controlled, double-blind pilot study. Nutrients. 2018;10(3):1-16.
doi pubmed - Lothian JB, Grey V, Lands LC. Effect of whey protein to modulate immune response in children with atopic asthma. Int J Food Sci Nutr. 2006;57(3-4):204-211.
doi pubmed - Gammone MA, Riccioni G, Parrinello G, D'Orazio N. Omega-3 polyunsaturated fatty acids: benefits and endpoints in sport. Nutrients. 2018;11(1):1-16.
doi pubmed - Lewis EJ, Radonic PW, Wolever TM, Wells GD. 21 days of mammalian omega-3 fatty acid supplementation improves aspects of neuromuscular function and performance in male athletes compared to olive oil placebo. J Int Soc Sports Nutr. 2015;12:28.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.