

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 2, Number 2, April 2010, pages 102-104
Syringomyelia: A Complication of an Underlying Pathology
Mohammad Sami Walida, c, Mazen Sanoufaa, Juan Salvatierrab
aMedical Center of Central Georgia, Macon, Georgia, USA
bMercer University, Macon, Georgia, USA
cCorresponding author, Email:
Manuscript accepted for publication April 06, 2010
Short title: Syringomyelia
doi: https://doi.org/10.4021/jocmr2010.04.291w
| Abstract | ▴Top |
Patients with syringomyelia may have diverse etiology and experience a variety of symptoms. This report describes two cases of syringomyelia in patients with different profiles, presentations and pathomechanisms.
Keywords: Syrigomyelia; Syrinx; Arachnoid cyst; Arnold-Chiari
| Introduction | ▴Top |
Syringomyelia (syrinx) is a rare neurological disorder characterized by slowly developing fluid-filled areas that extend longitudinally down the spinal cord causing symptoms such as pain, weakness and stiffness in the back, shoulders, arms, and legs. Syringomyelia has a prevalence of 3.3 to 8.5/100,000 people with some ethnic variability [1-4]. In the United States, syringomyelia is more common in African-Americans than in Caucasians [5]. Patients may have diverse etiology and experience a variety of symptoms. This report describes two cases of syringomyelia in patients with different profiles, presentations and pathomechanisms.
| Case 1 | ▴Top |
A 67-year-old Caucasian male presents with a history of worsening leg numbness of several years duration. Imaging showed a T4-T8 syrinx. An arachnoidal cyst was suspected at T6 due to the flattening and anterior displacement of the cord immediately under the spinal cord enlargement (Fig. 1). The patient had no remarkable medical history and was on no medications. He denied bowel or bladder symptoms. He smoked cigarettes and drank alcohol daily. Neurological exam was unremarkable except for some decreased sensation to light touch below L1. The patient underwent T4 to T8 posterior decompression and exploration with removal of arachnoidal cyst and opening of syrinx.
 Click for large image | Figure 1. Computed tomography with contrast (a 67-year-old male patient). |
| Case 2 | ▴Top |
A 12-year-old African-American girl presented with progressively worsening headaches. Neurological exam was unremarkable. Imaging showed a Chiari I deformity (low-lying cerebellar tonsils down to the level of C2) with a huge spinal cord syrinx from C2 to T2 (Fig. 2). Magnetic resonance angiography showed Limited flow through foramen magnum of the cerebrospinal fluid. The patient had posterior fossa craniotomy, C1-2 laminectomy and duraplasty for decompression of Chiari and midline cervical myelotomy for decompression and drainage of cervical syrinx.
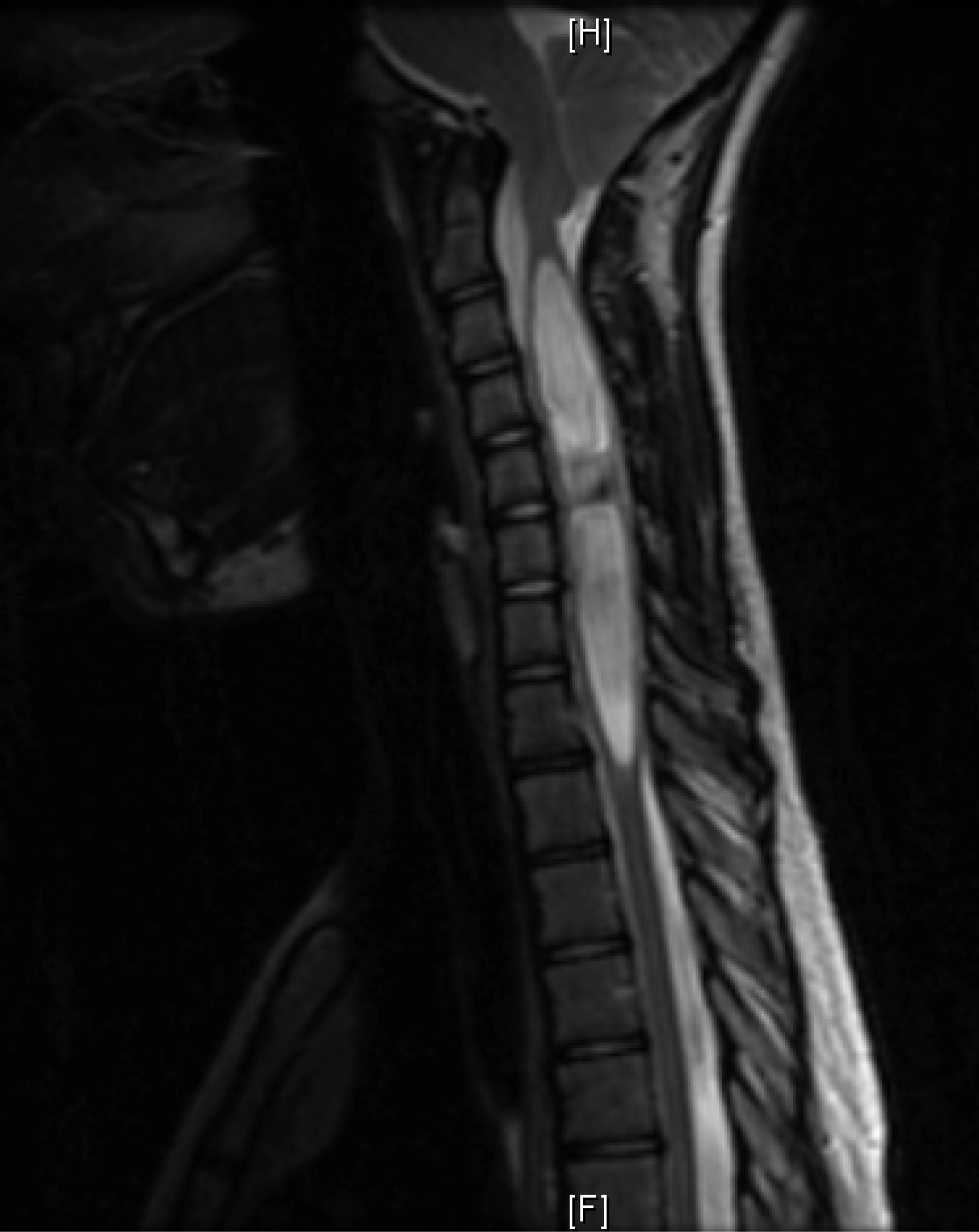 Click for large image | Figure 2. Magnetic resonance T2 image (a 12-year-old female patient). |
| Discussion | ▴Top |
Syringomyelia may be related to a congenital malformation or de novo abnormality in the central nervous system. Arachnoid cysts are intra-arachnoid collections of cerebrospinal fluid congenital in origin, however, onset of symptoms may be delayed until adolescence through expansion and pressure on the normal neural tissue leading to obstruction of the cerebrospinal fluid flow and neurological deficit [6]. These cysts may rarely be associated with syringomyelia or compressive myelopathy [7-9]. Spinal arachnoid cyst associated with syringomyelia can be treated by simple excision of the cyst without shunting the syrinx if the decompression effect resulting from removal of the cyst is sufficient [10].
Chiari malformation is another congenital abnormality whereby the cerebrellar tonsils herniate through the foramen magnum into the spinal canal causing disturbance in cerebrospinal fluid dynamics which may manifest by headaches, double vision, dizziness, and muscle weakness, particularly in the upper extermities. Most cases of non-traumatic syringomyelia occur in association with a Chiari malformation [11]. Very rarely both malformations (arachnoid cyst and Chiari malformation) can exist in a patient with syringomyelia [12, 13]. In most published cases the syringomyelia has been attributed to obstruction of cerebrospinal fluid flow at the foramen magnum by the arachnoid cyst itself. Very rarely, a posterior fossa arachnoid cyst may produce tonsillar descent and syringomyelia [12, 14].
Syringomyelia can be viewed as a complication of an underlying pathology which may be a simple arachnoid cyst or a complex Chiari malformation. It is important to keep these two entities in mind when dealing with patients expressing symptoms suggestive of progressive myelopathy in all age groups.
| References | ▴Top |
- Brewis M, Poskanzer DC, Rolland C, Miller H. Neurological disease in an English city. Acta Neurol Scand. 1966;42(Suppl 24):21-89.
pubmed - Brickell KL, Anderson NE, Charleston AJ, Hope JK, Bok AP, Barber PA. Ethnic differences in syringomyelia in New Zealand. J Neurol Neurosurg Psychiatry. 2006;77(8):989-991.
pubmed - Gudmundsson KR. The prevalence of some neurological diseases in Iceland. Acta Neurol Scand. 1968;44(1):57-69.
pubmed - Kurland LT. Descriptive epidemiology of selected neurologic and myopathic disorders with particular reference to a survey in Rochester, Minnesota. J Chronic Dis. 1958;8(4):378-418.
pubmed - Tipton AC
Jr. , Haerer AF. Syringomyelia in Mississippi. J Miss State Med Assoc. 1970;11(10):533-537.
pubmed - Gelabert-Gonzalez M. [Intracranial arachnoid cysts]. Rev Neurol. 2004;39(12):1161-1166.
pubmed - Ergun T, Lakadamyali H. Multiple extradural spinal arachnoid cysts causing diffuse myelomalacia of the spinal cord. Neurologist. 2009;15(6):347-350.
pubmed - Kim MS, Kim SH. Syringomyelia associated with a spinal arachnoid cyst. J Korean Neurosurg Soc. 2009;45(5):315-317.
pubmed - Kiran NA, Kasliwal MK, Suri A, Mahapatra AK. Giant posterior fossa arachnoid cyst associated with syringomyelia. Clin Neurol Neurosurg.
pubmed - Takeuchi A, Miyamoto K, Sugiyama S, Saitou M, Hosoe H, Shimizu K. Spinal arachnoid cysts associated with syringomyelia: report of two cases and a review of the literature. J Spinal Disord Tech. 2003;16(2):207-211.
pubmed - Owler BK, Halmagyi GM, Brennan J, Besser M. Syringomyelia with Chiari malformation; 3 unusual cases with implications for pathogenesis. Acta Neurochir (Wien). 2004;146(10):1137-1143, discussion 1143.
pubmed - Martinez-Lage JF, Almagro MJ, Ros de San Pedro J, Ruiz-Espejo A, Felipe-Murcia M. Regression of syringomyelia and tonsillar herniation after posterior fossa arachnoid cyst excision. Case report and literature review. Neurocirugia (Astur). 2007;18(3):227-231.
pubmed - Martinez-Lage JF, Ruiz-Espejo A, Guillen-Navarro E, Almagro MJ. Posterior fossa arachnoid cyst, tonsillar herniation, and syringomyelia in trichorhinophalangeal syndrome Type I. J Neurosurg. 2008;109(4):746-750.
pubmed - Bauer AM, Mueller DM, Oro JJ. Arachnoid cyst resulting in tonsillar herniation and syringomyelia in a patient with achondroplasia. Case report. Neurosurg Focus. 2005;19(5):E14.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.