Figures
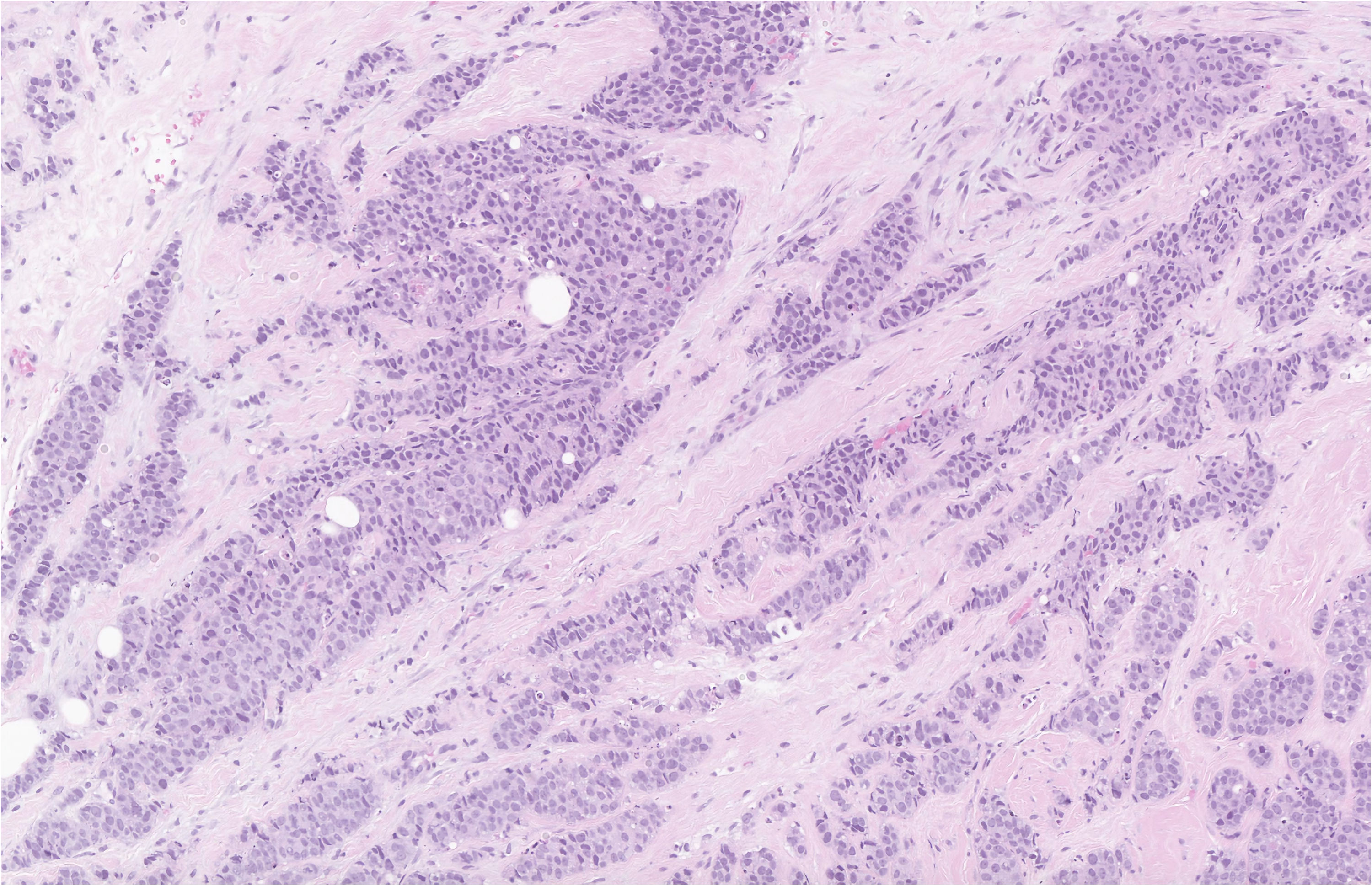
Figure 1. Hematoxylin and eosin stain of the breast biopsy demonstrating IDC with a nuclear grade of 3 at low power. The myoepithelial layer is lost and the tubuloglandular architecture seen in benign breast tissue is not preserved.
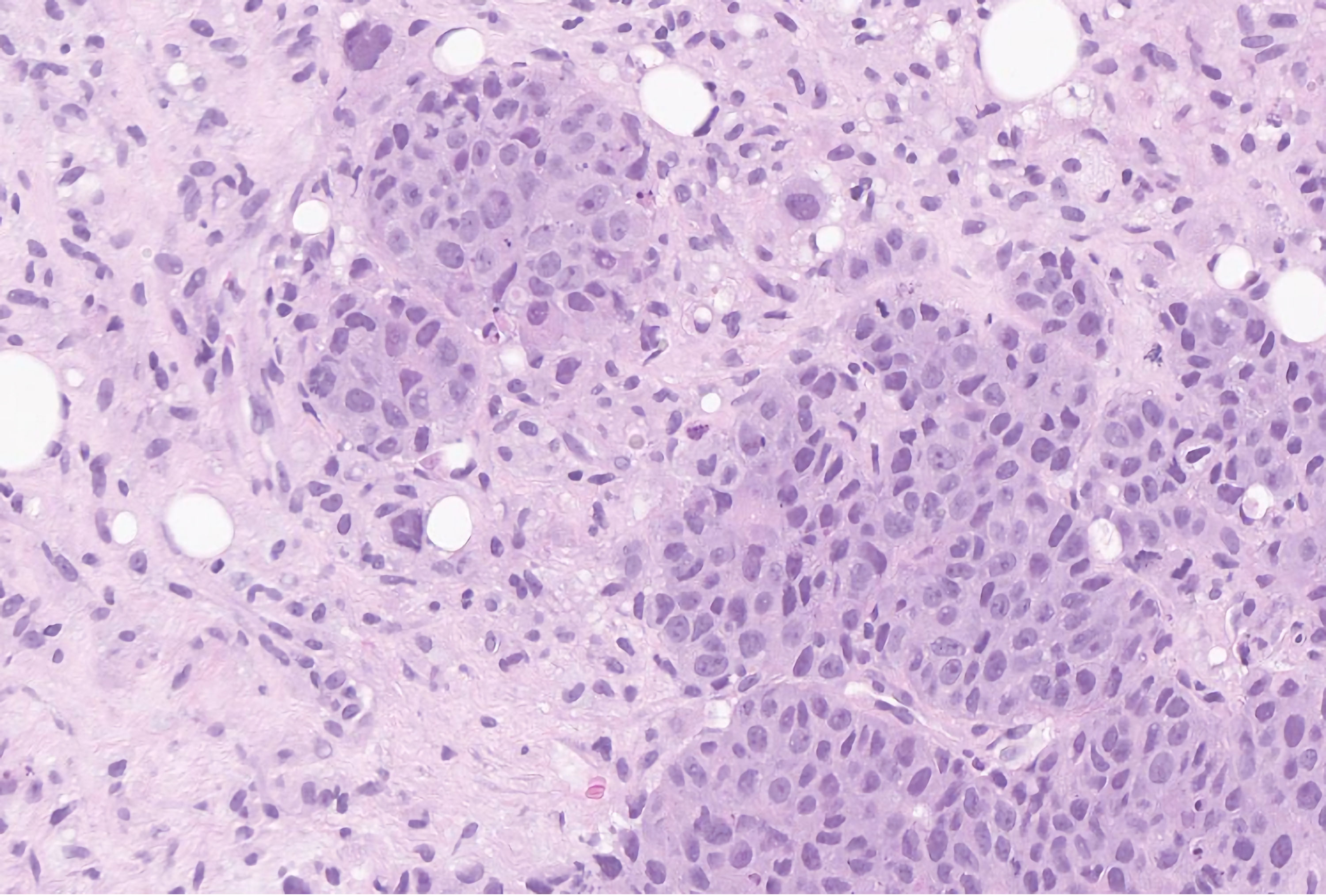
Figure 2. Hematoxylin and eosin stain of the breast biopsy demonstrating invasive carcinoma of no special type, with a nuclear grade of 3 at high power. The cells have bizarre shapes and sizes with prominent nuclei and hyperchromatic chromatin. GATA-3 and mammaglobin stained positively in the tumor cells, consistent with a breast primary.
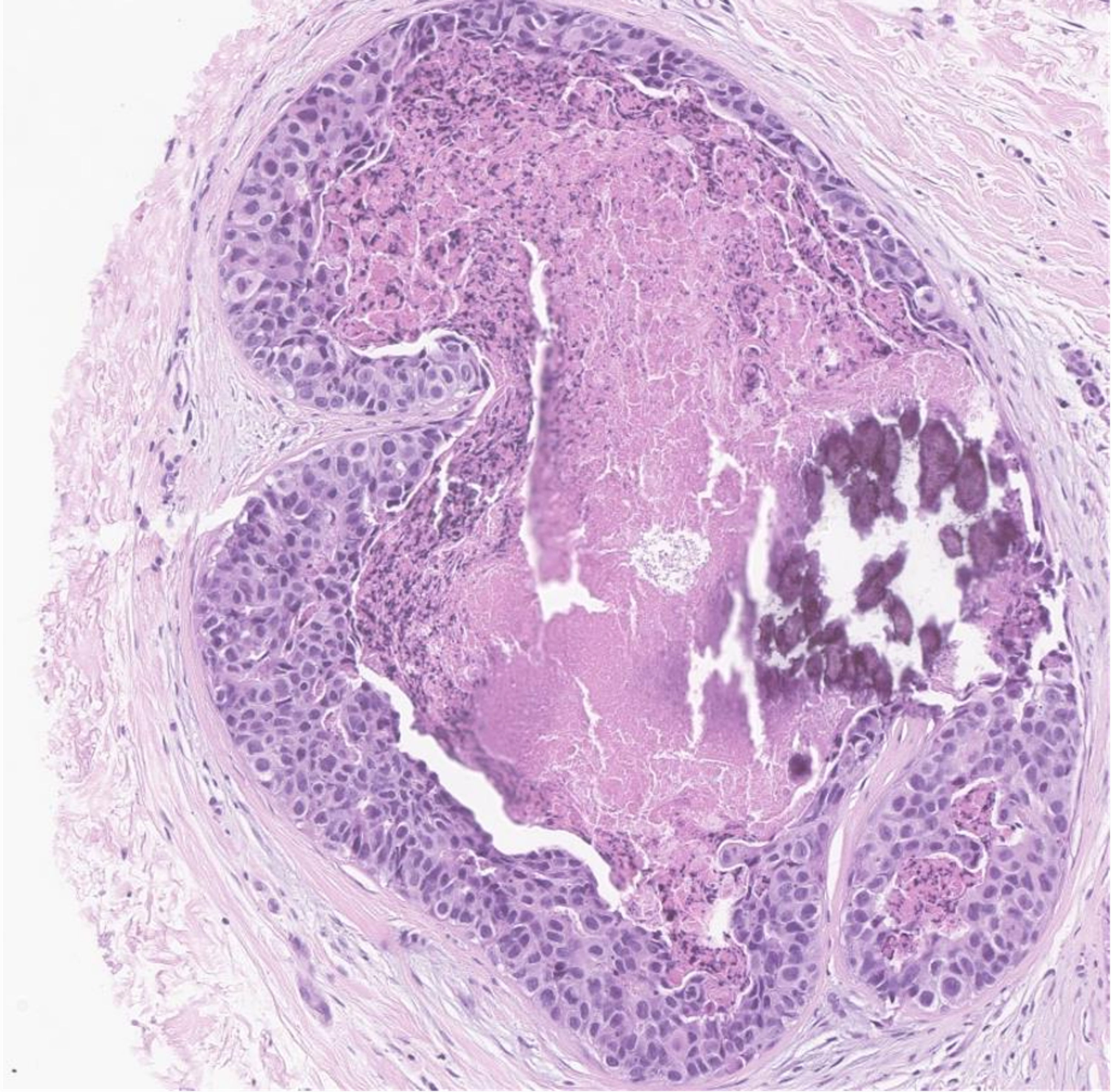
Figure 3. Hematoxylin and eosin stain of the breast biopsy demonstrating ductal carcinoma in situ with nuclear grade 3 at medium power. This patient had carcinoma with comedo and solid histological patterns, in addition to comedonecrosis and calcifications. The myoepithelial layer is maintained. The cells themselves are moderately pleomorphic with hyperchromatic chromatin.
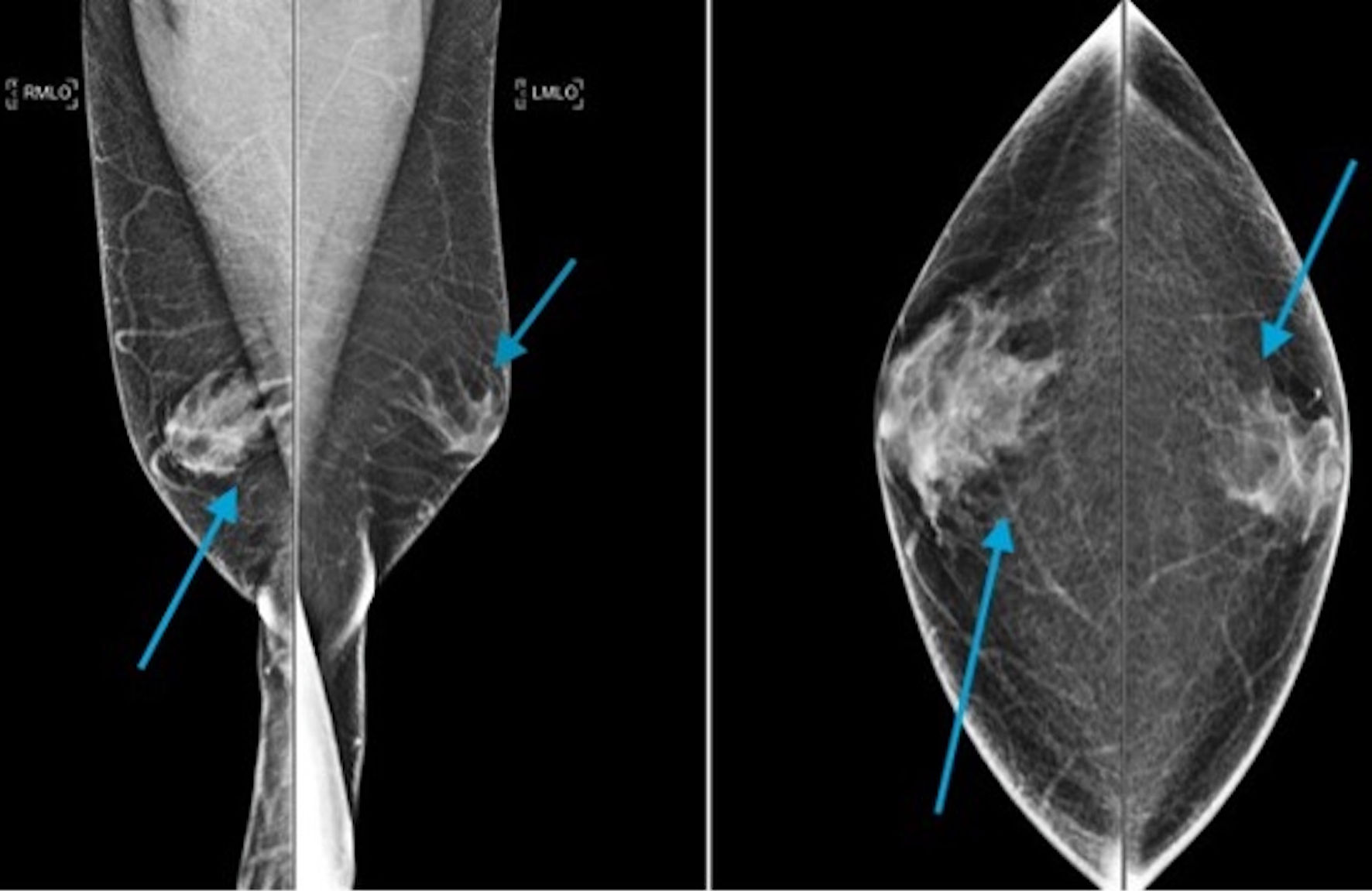
Figure 4. A mediolateral oblique digital mammogram demonstrating irregular flamed shaped structure within the subareolar region of the right breast extending into the adjacent fat, characteristic of gynecomastia (arrow heads). This is greater on the right than on the left side.
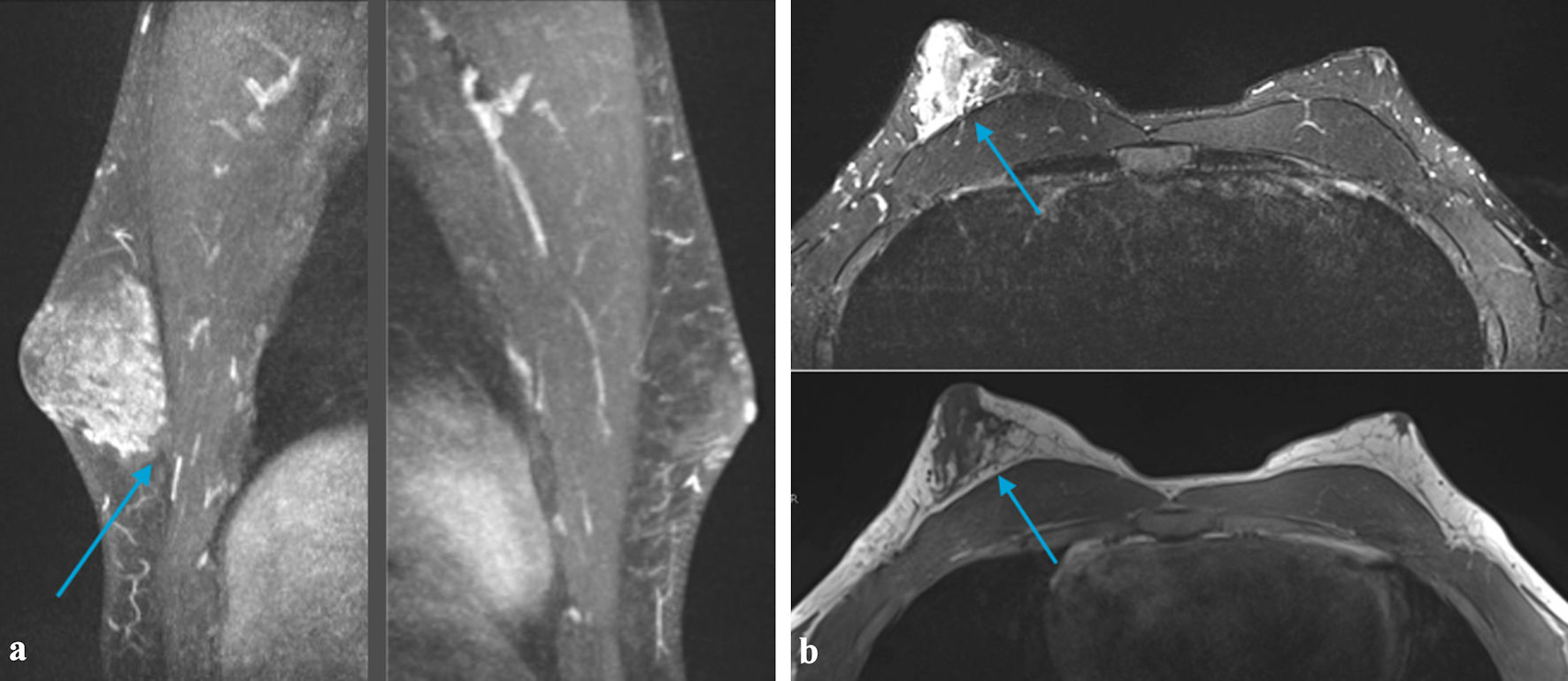
Figure 5. (a) MRI of the breast demonstrating a small area of heterogeneous tissue beneath the left areola. There is an asymmetrically larger amount of heterogeneous tissue within the subareolar region of the right breast extending into the central breast (arrow). These findings are suggestive of gynecomastia (This could be related to an underlying germ cell tumor and/or medications). No suspicious area of mass was identified within either breast. (b) MRI of the breast demonstrating small area of heterogeneous tissue beneath the left areola. There is an asymmetrically larger amount of heterogeneous tissue within the subareolar region of the right breast extending into the central breast (arrow). These findings are suggestive of gynecomastia (This could be related to an underlying germ cell tumor and/medications). No suspicious area of mass was identified within either breast. MRI: magnetic resonance imaging.
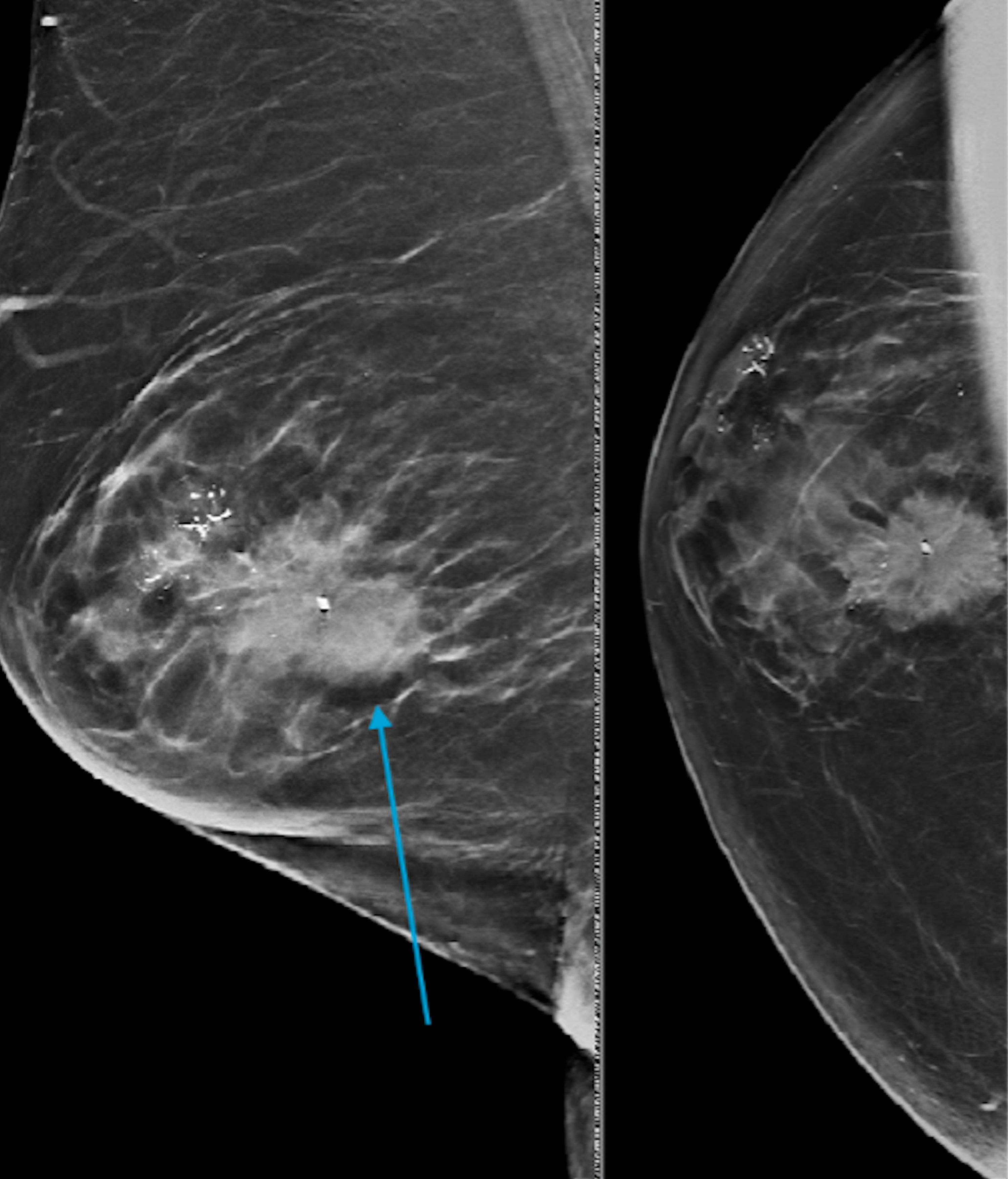
Figure 6. Bilateral diagnostic mammogram demonstrating an irregular mass with pleomorphic calcification in the right breast at 10:00 o’clock position (arrow) and 12:00 o’clock position. Moderate gynecomastia is present in the left breast. Biopsy of the mass at 10:00 o’clock revealed ductal carcinoma in situ and 12:00 o’clock revealed invasive ductal carcinoma.
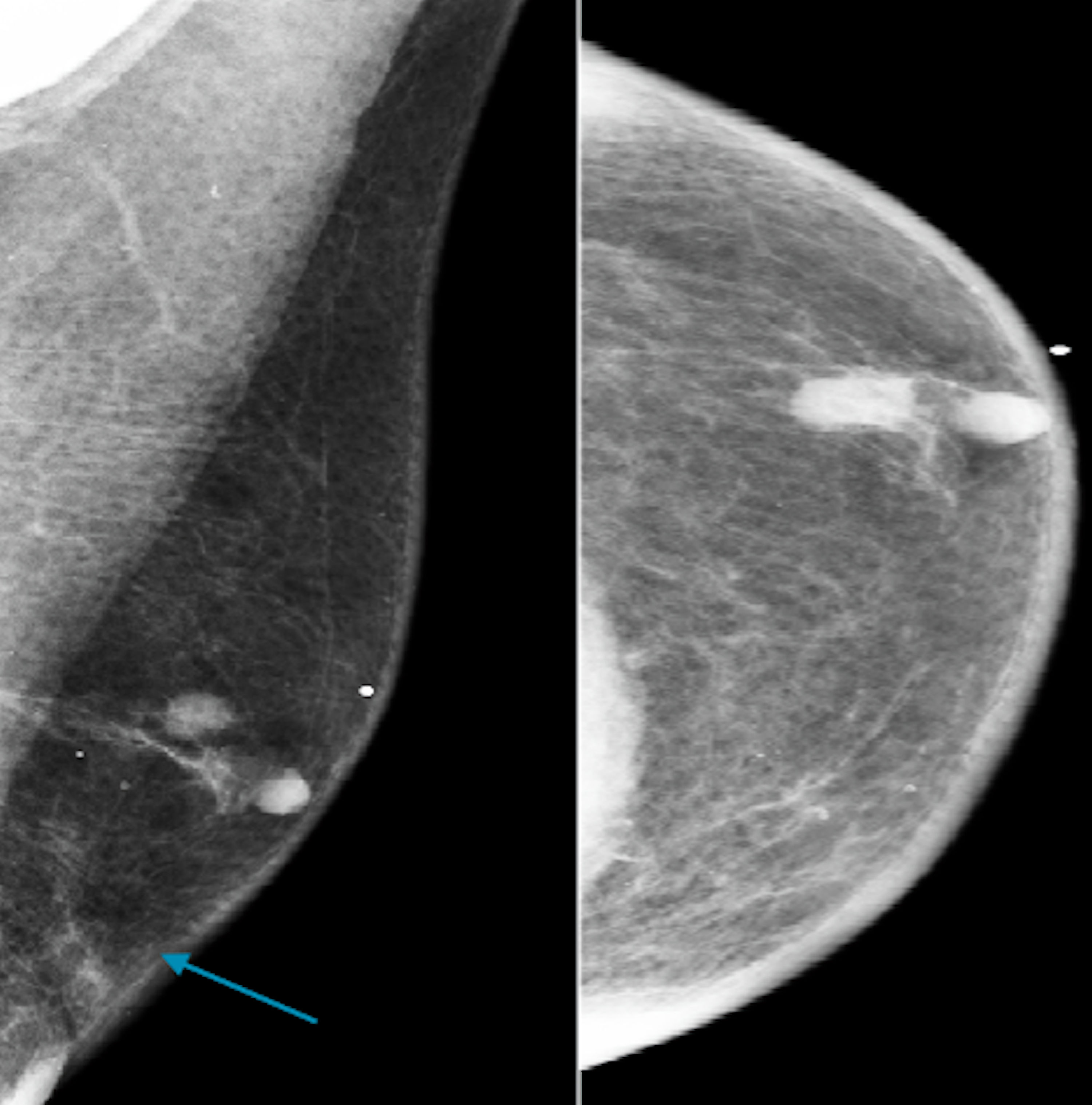
Figure 7. Craniocaudal and mediolateral oblique digital mammogram demonstrating scattered areas of fibro-glandular density and a suspicious mass (blue arrow) at 12:00 o’clock of the left breast according to BI-RADS 4. BIRADS: the Breast Imaging Reporting and Data System.
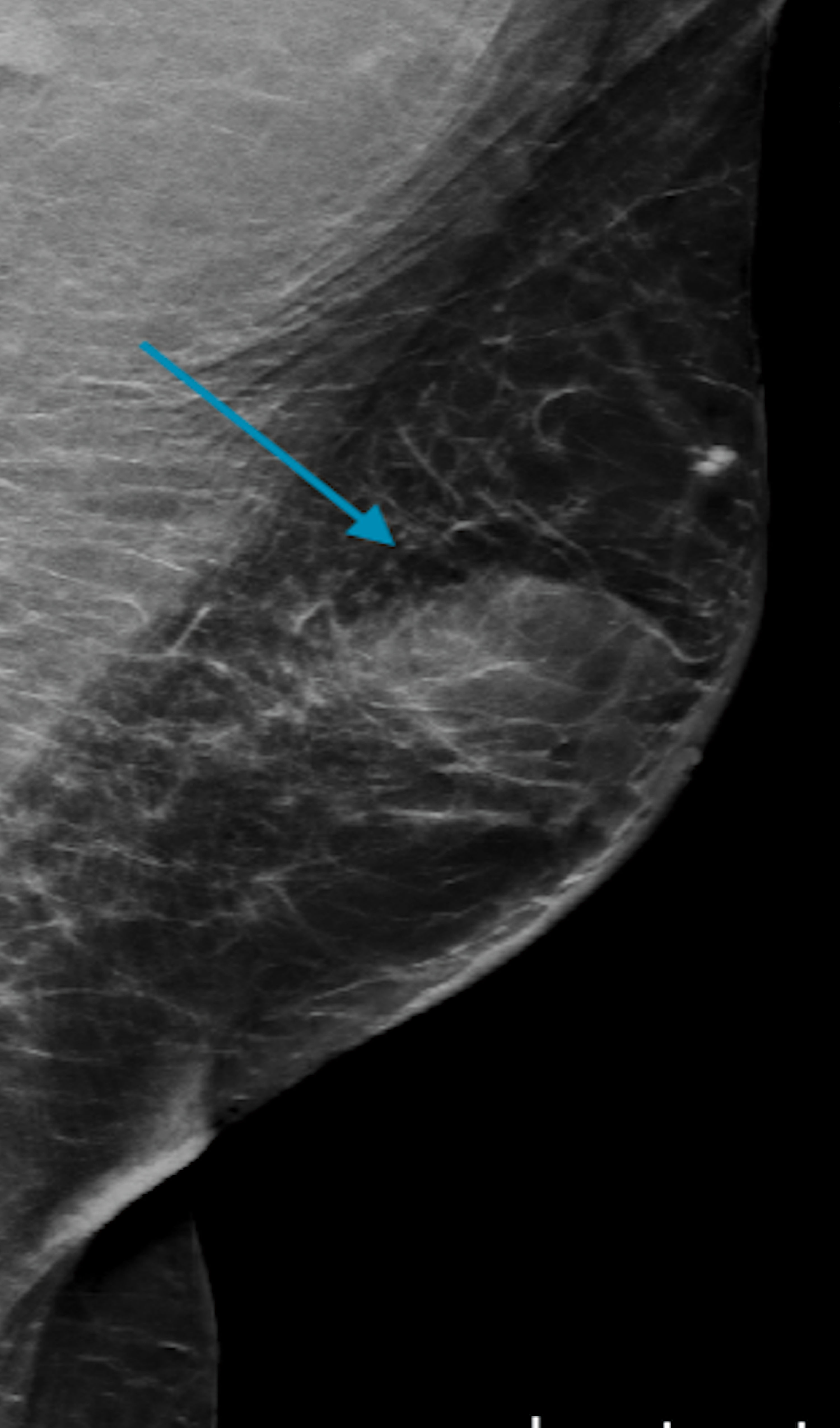
Figure 8. A mediolateral oblique digital mammogram illustrating a partially circumscribed indistinct mass in the central left breast (blue arrow).
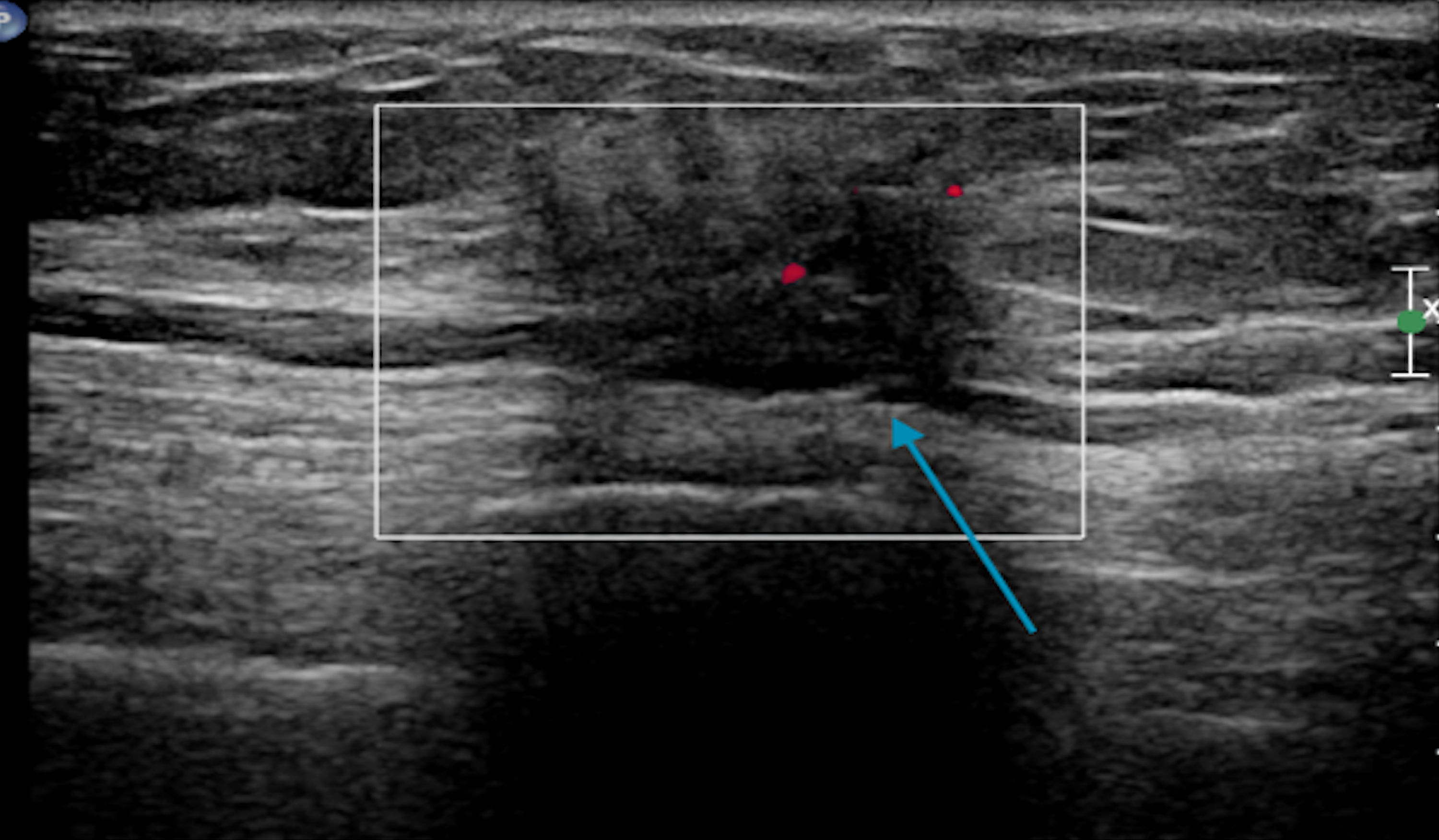
Figure 9. Targeted sonogram of the left breast showing a 1.1 × 0.7 × 0.8 cm irregular nonparallel spiculated hypoechoic mass with posterior shadowing (blue arrow).
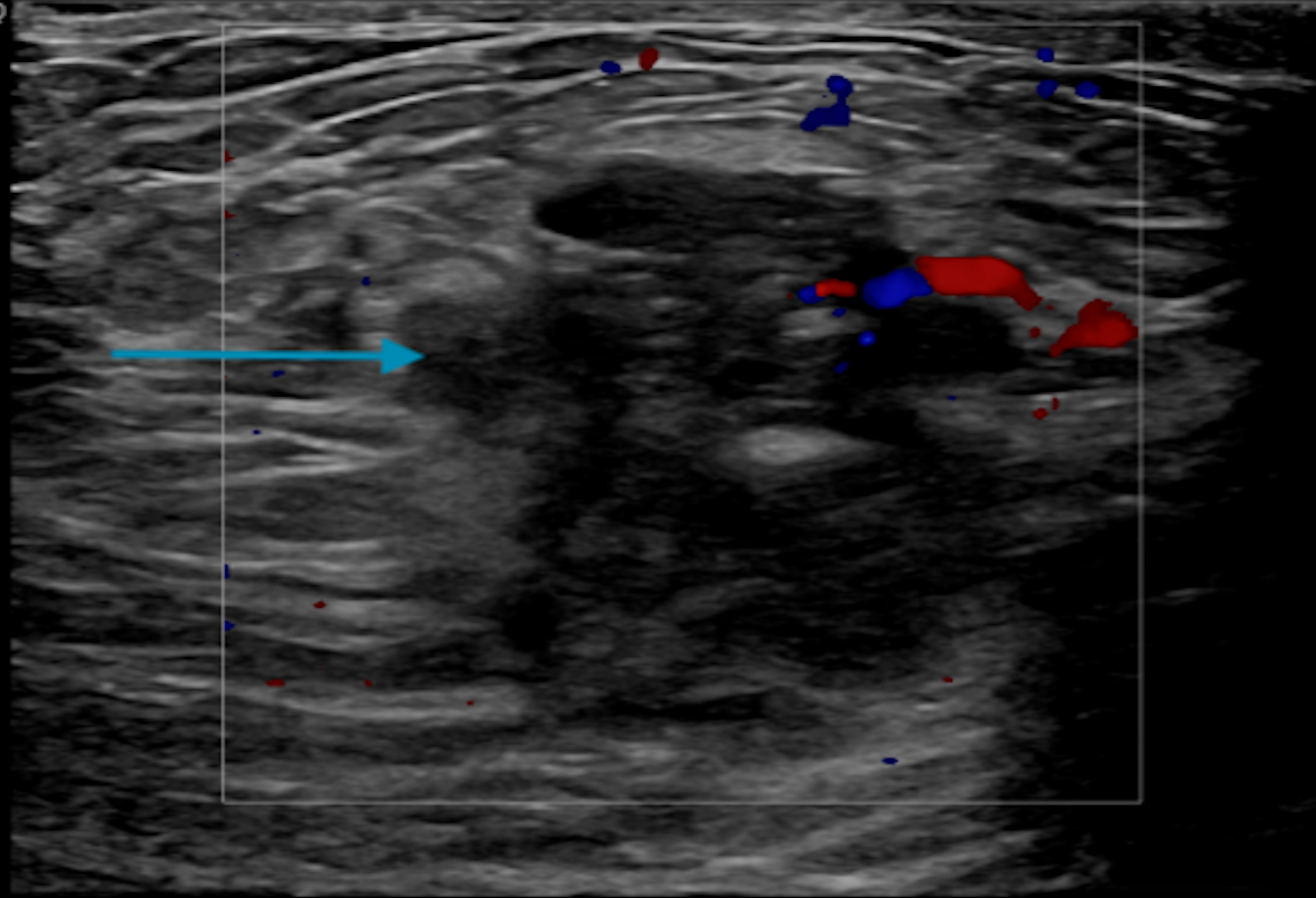
Figure 10. Single transverse image ultrasound of the right breast demonstrating an irregular 2.5 × 1.3 × 3 cm mass at 12:00 o’clock position and a 3.1 × 0.5 × 1.2 cm hypoechoic mass with calcifications at 10:00 o’clock position (blue arrow).
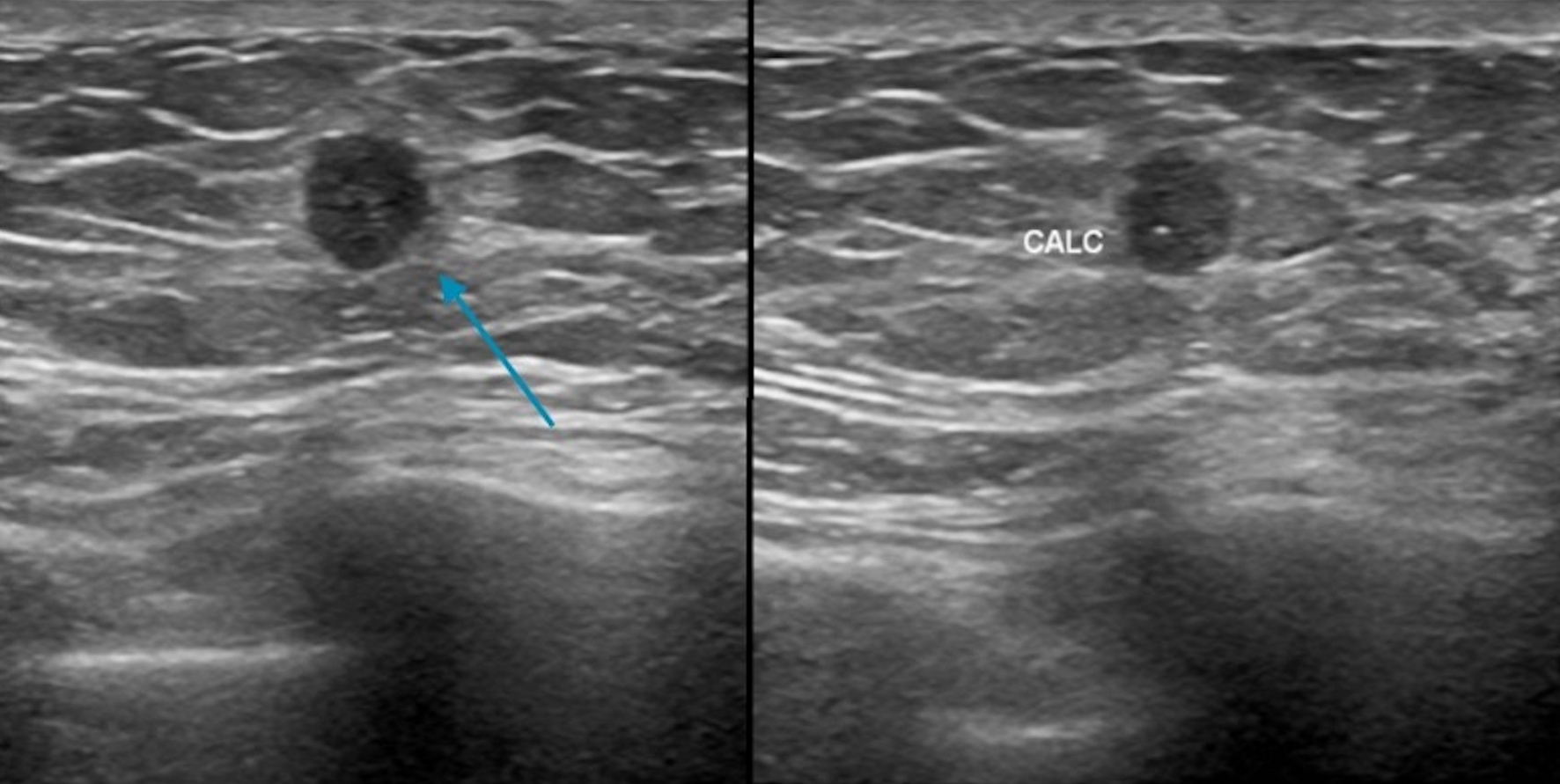
Figure 11. Ultrasound demonstrating a circumscribed mass (blue arrow) in the 12:00 o’clock position with calcifications. CALC: calcification.
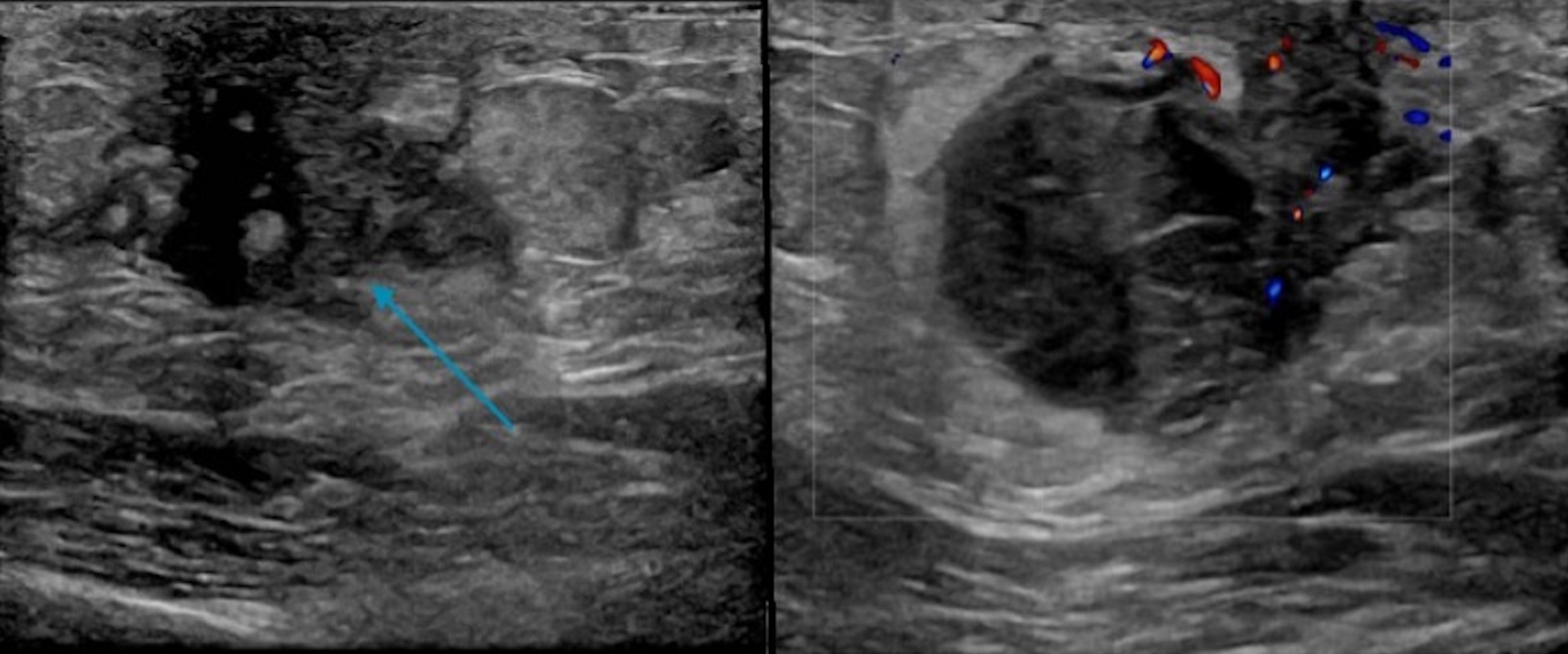
Figure 12. Targeted ultrasound displaying a 3.1 × 1.8 × 2.7 cm hypoechoic mainly circumscribed mass (blue arrow) behind the left nipple with mild surrounding edema (no left axillary lymphadenopathy).
Table
Table 1. Indications for MRI in Male Breast Cancer
| 1) Equivocal imaging findings [54] |
| 2) To evaluate the posterior extent of the disease, and skin and chest wall involvement [52] |
| 3) To evaluate for a primary breast mass in the setting of axillary metastasis and negative mammography and sonography [52] |
| 4) To evaluate for a primary breast mass in the setting of clinical diagnosis of inflammatory breast cancer and evaluation of potential skin involvement in a known malignancy when clinically suspicious [52] |
| 5) To evaluate for residual disease post-surgery [52] |