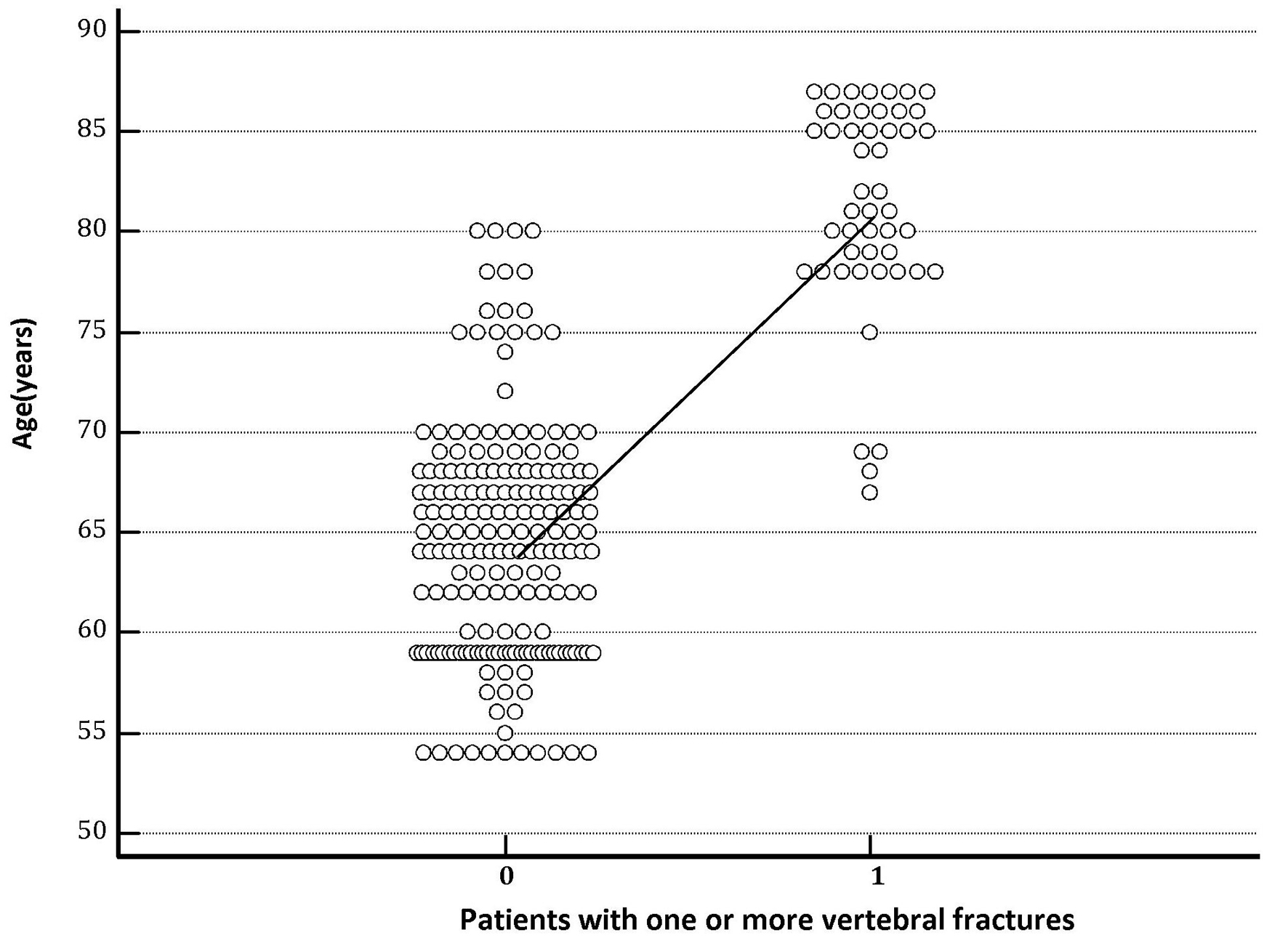
Figure 1. The column on the right represents the group of hypertensive patients who experienced one or more vertebral fractures during the follow-up. The graph clearly shows that mean age recorded at the entrance into the study was significantly higher (P < 0.001) in hypertensive patients with destructive osteoporosis of the spine, i.e., which developed one or more vertebral fractures (age 81.33 ± 5.27 years) compared with those that did not have vertebral collapses (age 64.53 ± 5.86 years).
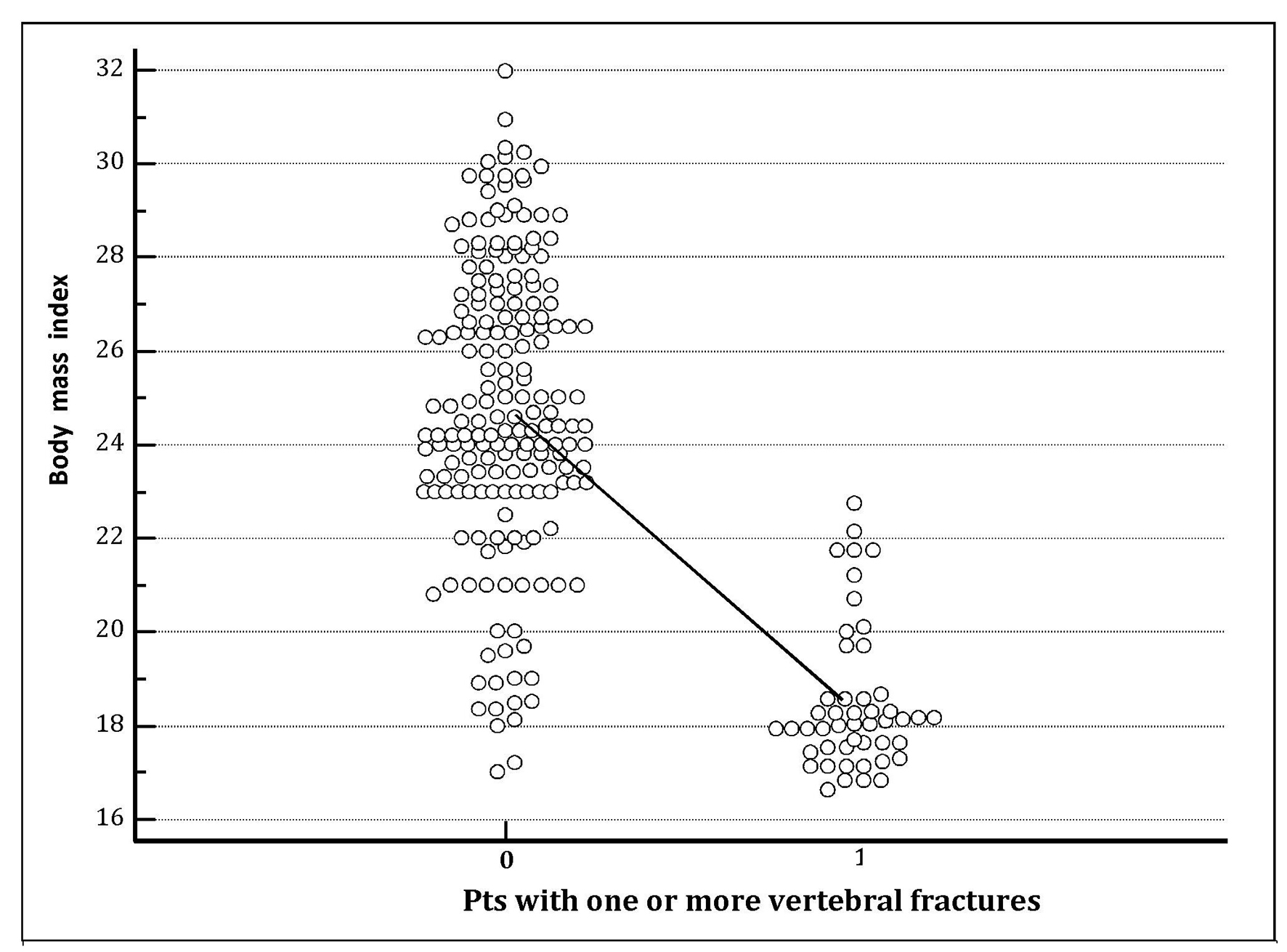
Figure 2. The column on the right represents the group of hypertensive patients who experienced one or more vertebral fractures during the follow-up. The chart clearly shows that mean body mass index (BMI) recorded at the entrance into the study was significantly lower (P < 0.001) in hypertensive patients with destructive osteoporosis of the spine, i.e., which developed one or more vertebral fractures (BMI 18.85 ± 1.52) compared with those that did not have vertebral collapses (BMI 24.86 ± 3.10).
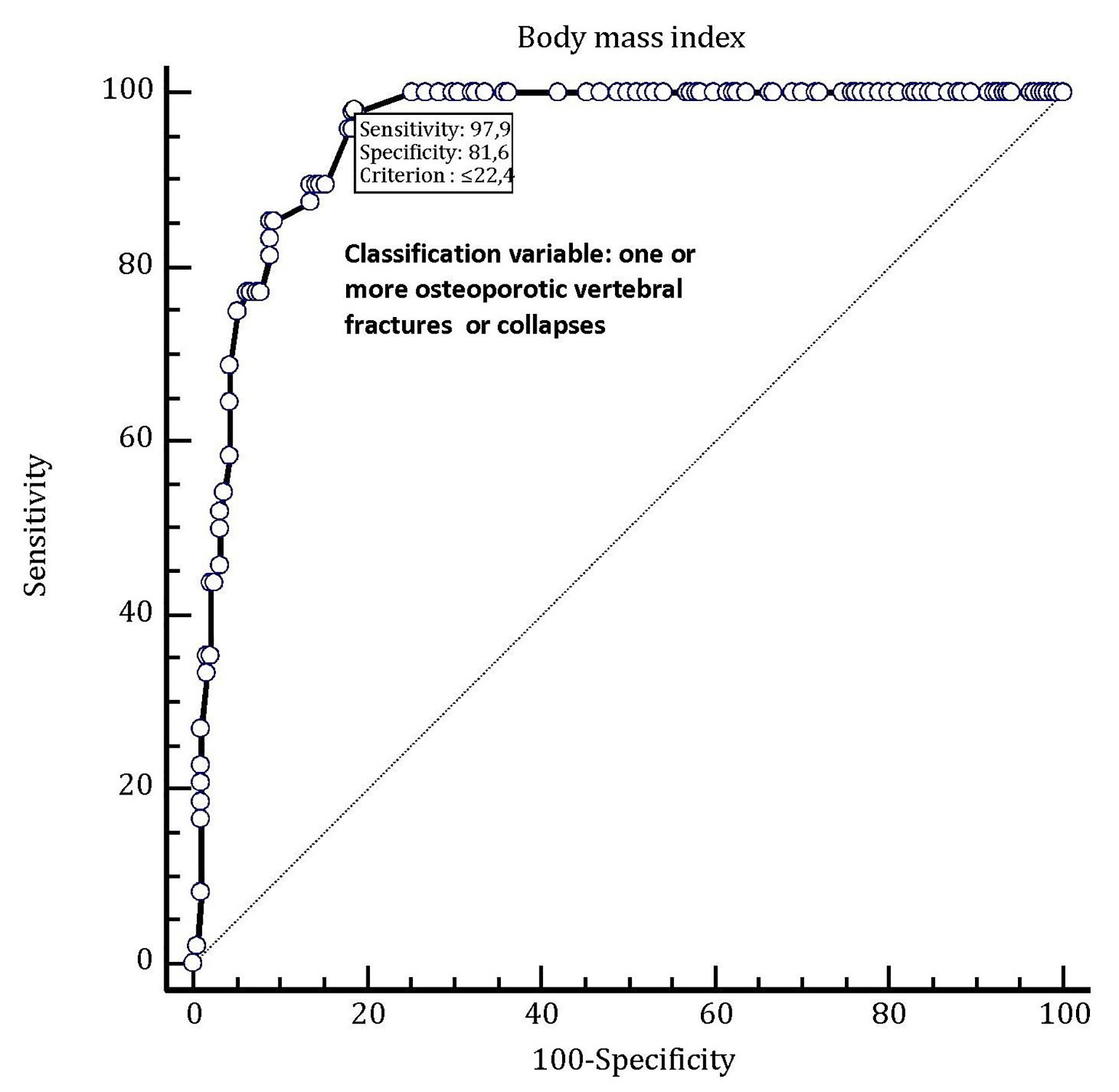
Figure 3. In this ROC plot, there is the representation of the very good predictive value (AUC = 0.950) possessed by body mass index (BMI) as a tool for predicting the occurrence of one or more osteoporotic vertebral fractures in hypertensive female patients older than 70 years taking chronic therapy with an oral thiazide diuretic (alone or in combination with another antihypertensive drug). By adopting this method, the best diagnostic accuracy for predicting an osteoporotic spinal fracture has been attributed to the BMI threshold value of 22.4. This means that in the enrolled population of thiazide users, this value is associated to the presence of osteoporotic vertebral collapse or fracture with a sensitivity of 97.9% and a specificity of 81.6% (note on top of the graph).