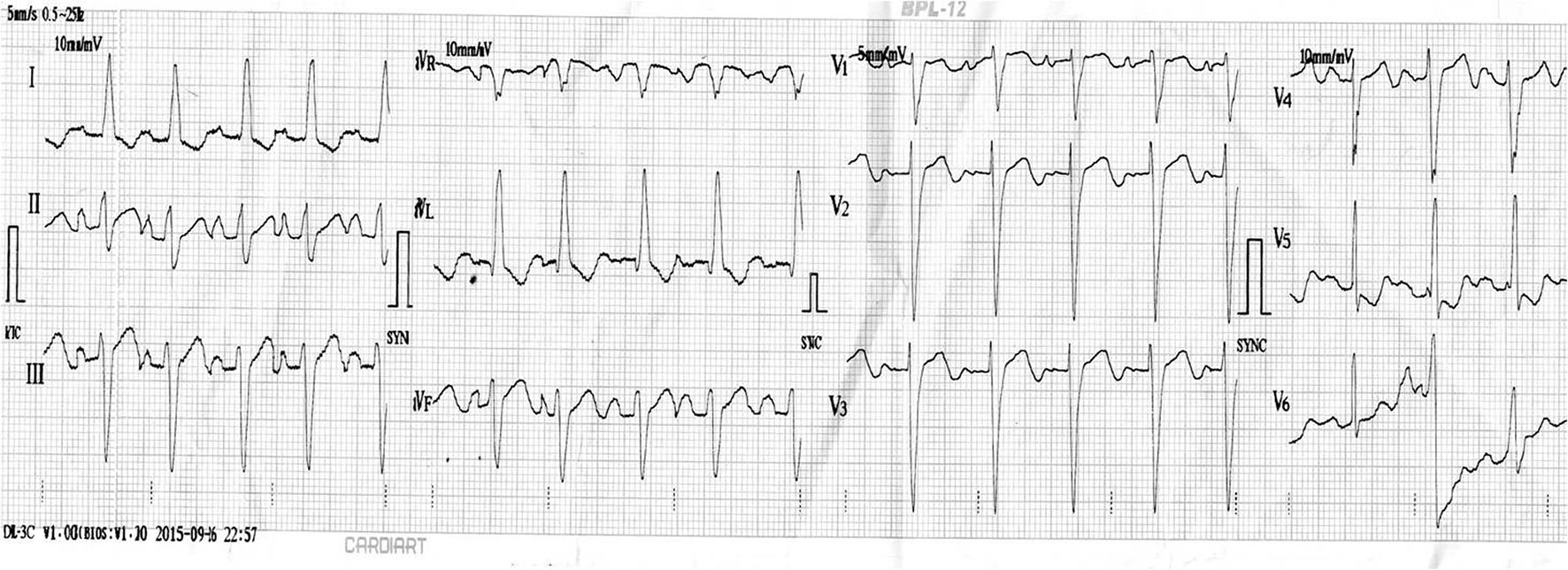
Figure 1. ECG displaying normal sinus rhythm, biatrial enlargement, left axis deviation, poor R progression and ST-T changes in leads V5-6.
| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 8, Number 10, October 2016, pages 760-763
Unusual Survival of Anomalous Left Coronary Artery From the Pulmonary Artery With Severe Rheumatic Mitral Stenosis in Septuagenarian Women: Foes Becoming Friends?
Figures